Last updated on Mar 26, 2016
Get the free Antipsychotics Prior Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Antipsychotics PA Form
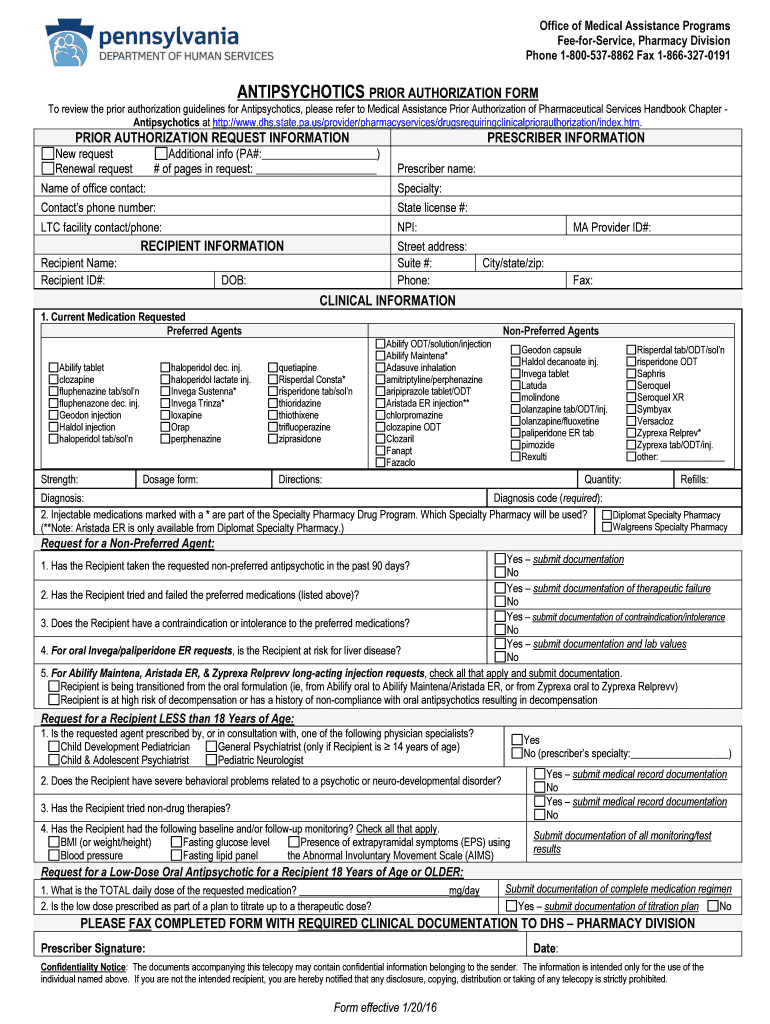
The Antipsychotics Prior Authorization Form is a medical consent document used by healthcare providers in Pennsylvania to request prior authorization for antipsychotic medications.
pdfFiller scores top ratings on review platforms
Who needs Antipsychotics PA Form?
Explore how professionals across industries use pdfFiller.

Antipsychotics PA Form is needed by:
-
Healthcare providers prescribing antipsychotic medications
-
Pharmacy staff processing prior authorization requests
-
Mental health professionals overseeing patient medication
-
Insurance companies evaluating medication authorization
-
Patients requiring antipsychotic medications under insurance plans
Comprehensive Guide to Antipsychotics PA Form
What is the Antipsychotics Prior Authorization Form?
The Antipsychotics Prior Authorization Form is a critical document used by healthcare providers in Pennsylvania to secure authorization for prescribing antipsychotic medications. This form plays a significant role in the healthcare system, ensuring that patients receive necessary medications while adhering to state regulations.
Its importance lies in the requirement for prescribers to gain approval before initiating treatment, which helps manage costs and maintains a framework for appropriate medication use.
Purpose and Benefits of the Antipsychotics Prior Authorization Form
The primary purpose of the Antipsychotics Prior Authorization Form is to facilitate the process by which healthcare providers obtain authorization for psychiatric medications. This process is essential in the context of mental health, where timely access to medication can significantly impact patient outcomes.
Utilizing this form provides numerous benefits, including streamlined medication approval for health practitioners, which can enhance the efficiency of patient care and reduce delays in treatment.
Who Needs the Antipsychotics Prior Authorization Form?
Several parties are involved in the prior authorization process for antipsychotic medications. Key individuals include prescribers and pharmacists, who play crucial roles in ensuring that the form is properly filled out and submitted.
Patients receiving antipsychotic treatment must meet specific eligibility criteria, which can vary based on their individual needs and the medications prescribed.
How to Fill Out the Antipsychotics Prior Authorization Form Online (Step-by-Step)
-
Access the form through pdfFiller's platform to begin the process.
-
Fill in the required fields with patient and prescriber information.
-
Gather necessary clinical details before finalizing the form, such as current medications and medical history.
-
Review the form for completeness and accuracy.
-
Submit the form electronically or via fax as per your preferred submission method.
Utilizing an online platform can significantly ease the process of completing clinical prior authorization forms for mental health medications.
Common Errors and How to Avoid Them
Filling out the Antipsychotics Prior Authorization Form can result in several common errors if care is not taken. Issues such as missing signatures and incorrect patient information are frequent pitfalls.
To avoid these mistakes, practitioners should develop a review and validation checklist to ensure all necessary details are included and accurate before submission.
Submission Methods for the Antipsychotics Prior Authorization Form
Once completed, the Antipsychotics Prior Authorization Form can be submitted through various methods. One common approach is faxing the form directly to the Department of Human Services (DHS) Pharmacy Division.
Additionally, electronic submission options may also be available, providing flexibility in how healthcare providers manage their prior authorization requests.
What Happens After You Submit the Antipsychotics Prior Authorization Form?
After submitting the Antipsychotics Prior Authorization Form, users can expect a confirmation of receipt from the appropriate authority. It is essential to be aware of potential processing times, which can vary depending on the department.
Healthcare providers should be informed about the possible outcomes of the prior authorization request, including approvals, denials, or requests for additional information.
Security and Compliance When Using the Antipsychotics Prior Authorization Form
When handling sensitive information via the Antipsychotics Prior Authorization Form, security and compliance are paramount. pdfFiller employs robust security measures, including HIPAA compliance and data encryption, to protect users' information.
Ensuring data protection is vital for both healthcare providers and patients, as it maintains trust and confidentiality in handling sensitive medical documents.
Utilizing pdfFiller for the Antipsychotics Prior Authorization Form
Using pdfFiller for the Antipsychotics Prior Authorization Form can greatly enhance the user experience. It allows for easy creation, filling, eSigning, and submission of forms without the need for downloads or complicated processes.
The platform features user-friendly tools for editing, annotating, and managing forms, making it an ideal choice for healthcare providers looking for efficiency in their documentation processes.
How to fill out the Antipsychotics PA Form
-
1.Start by visiting pdfFiller and searching for the Antipsychotics Prior Authorization Form in the form library.
-
2.Once located, open the form by clicking on it, which will enable you to access the editing features.
-
3.Before filling out the form, gather all necessary information, including recipient and prescriber details, current medication requests, and specific clinical data.
-
4.As you navigate the form, click on each field to input information using pdfFiller's user-friendly interface.
-
5.Ensure you complete all required fields marked with an asterisk to avoid delays in processing.
-
6.Review each section thoroughly to confirm accuracy and completeness, using pdfFiller's built-in tools to check for any missing information.
-
7.Once you are satisfied with the form, use the 'Sign' option to electronically sign, ensuring the prescriber’s signature is included.
-
8.Finally, save your completed form using the 'Save' option, and download the document to submit it or choose to fax it directly through the pdfFiller interface.

Who is eligible to submit the Antipsychotics Prior Authorization Form?
Eligible submitters are healthcare providers and prescribers in Pennsylvania who are authorized to request prior authorization for antipsychotic medications on behalf of their patients.
What supporting documents are required with the form?
Typically, prescribers need to include relevant clinical data, patient health records related to the antipsychotic treatment, and any previous medication history that supports the authorization request.
What is the process for submitting the Antipsychotics Prior Authorization Form?
Submit the completed form by faxing it to the DHS Pharmacy Division, making sure to follow any submission guidelines specified by the insurance provider related to prior authorization requests.
Are there any common mistakes to avoid when completing this form?
Common mistakes include omitting required fields, failing to provide a prescriber’s signature, and not double-checking for accurate clinical data. Ensure all information is current and complete.
How long does it take to process the prior authorization request?
Processing times can vary; typically, it takes several business days. Ensure that the request is submitted well in advance of the patient needing the medication to avoid delays.
What happens if the prior authorization is denied?
In cases of denial, prescribers can appeal the decision. It's important to gather additional information or documentation that supports the medical necessity of the medication.
Can patients directly submit the Antipsychotics Prior Authorization Form?
No, patients cannot submit the form directly. It must be completed and submitted by the healthcare provider or prescriber responsible for their care.
Related Forms









Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.