Last updated on Mar 26, 2016
Get the free Medical History Questionnaire
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medical History Form
The Medical History Questionnaire is a document used by patients to provide comprehensive medical and personal information to healthcare providers for eye care.
pdfFiller scores top ratings on review platforms
Who needs Medical History Form?
Explore how professionals across industries use pdfFiller.

Medical History Form is needed by:
-
Patients seeking eye care services
-
Healthcare providers at eye clinics
-
Medical professionals conducting patient intake
-
Insurance companies requiring medical history for claims
-
Administrative staff managing patient records
-
Individuals assisting seniors or patients with form completion
Comprehensive Guide to Medical History Form
What is the Medical History Questionnaire?
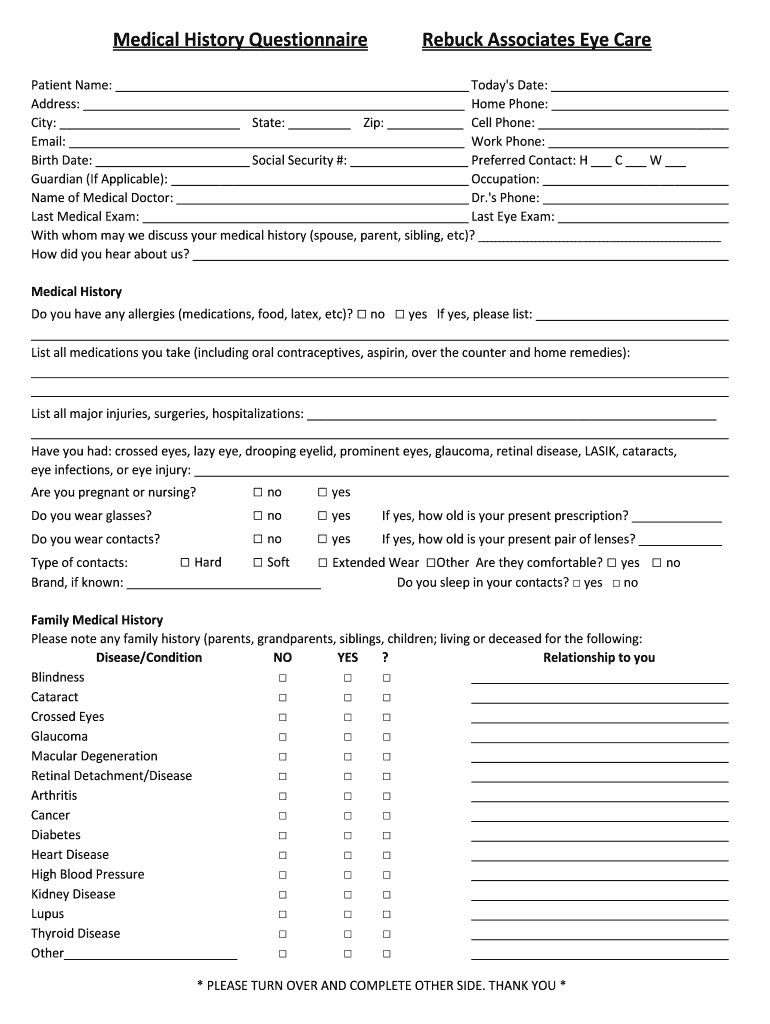
The Medical History Questionnaire is a vital healthcare intake form used by Rebuck Associates Eye Care. This document is designed to gather essential health data from patients, ensuring that healthcare providers have a comprehensive understanding of their medical background. Key sections included in the form cover personal details, medical history, and family history, allowing for accurate assessments and tailored treatments.
Purpose and Benefits of the Medical History Questionnaire
Completing the Medical History Questionnaire is crucial for patients seeking eye care services. Collecting accurate medical history enhances the quality of care provided, leading to better eye health outcomes. A comprehensive health record from this health history form enables healthcare providers to make informed treatment decisions and consult effectively with patients, thus optimizing the consultation process.
Key Features of the Medical History Questionnaire
This medical questionnaire template includes several important features that enhance its effectiveness:
-
Sections detailing allergies, medications, surgeries, and eye conditions.
-
Fillable form format with checkboxes and blank fields for user convenience.
-
Policies that require patient signatures for consent and acknowledgment.
Who Needs the Medical History Questionnaire?
The Medical History Questionnaire is essential for all patients seeking eye care services at Rebuck Associates Eye Care. Both new and returning patients are required to complete the form, particularly in scenarios such as pre-exams or prior to new treatments. This ensures that healthcare providers have accurate and up-to-date information to deliver the best possible care.
How to Fill Out the Medical History Questionnaire Online
To complete the Medical History Questionnaire using pdfFiller, follow these steps:
-
Access the form online via the pdfFiller platform.
-
Gather necessary medical information before starting to ensure accuracy.
-
Navigate through each section carefully, filling out all required fields.
Common Errors and How to Avoid Them
While filling out the patient medical form, it's important to avoid common mistakes. Potential pitfalls include incomplete sections or providing incorrect information. Reviewing the form before submission is crucial for accuracy, so create a validation checklist to ensure that all required information is complete and correct.
How to Sign the Medical History Questionnaire
Signing the Medical History Questionnaire can be done digitally or with a wet signature. To eSign the form using pdfFiller, follow these instructions:
-
Select the digital signature option within the pdfFiller platform.
-
Follow the prompts to add your signature electronically.
Understanding the legal implications of signing, including the assignment and release section, is essential for compliance and acknowledgment.
Submitting the Medical History Questionnaire
Once completed, the Medical History Questionnaire can be submitted in several ways:
-
Online through the pdfFiller platform.
-
Printed and submitted in person.
-
Sent via mail to the designated healthcare facility.
After submission, it's advisable to follow up to confirm that the form has been received.
Security and Compliance for the Medical History Questionnaire
Data protection is a priority when handling the Medical History Questionnaire. PdfFiller employs robust security features, including encryption standards that align with HIPAA and GDPR compliance. This ensures that sensitive health information remains private and secure throughout the handling process.
Get Started with Your Medical History Questionnaire
Using pdfFiller simplifies the process of filling out the Medical History Questionnaire, enhancing your overall healthcare experience. Start the form today and take the first step towards better eye care, with additional resources available through pdfFiller to assist you along the way.
How to fill out the Medical History Form
-
1.To access the Medical History Questionnaire on pdfFiller, visit the pdfFiller website and use the search bar to find the form by its name.
-
2.Once the form is opened, carefully read through the instructions provided at the top to understand what information is required.
-
3.Gather necessary information beforehand, including personal details, medical history, family medical history, allergies, medications, past surgeries, and any eye conditions.
-
4.Navigate through the form fields using your mouse or keyboard. Click on each blank field to type in the required information or select options from checkboxes.
-
5.Make sure to complete each section methodically; the form includes segments for personal, medical, and family history that need to be filled out accurately.
-
6.After filling in all necessary fields, review the form carefully to ensure all information is correct. Check for any missed fields or errors.
-
7.Once satisfied with your entries, you have options to save or download the form. Click the 'Save' button or select 'Download' to keep a copy for your records.
-
8.If required, complete the signature section by clicking on the designated signature field, and sign using your mouse or trackpad.
-
9.Finally, submit the form as directed by your healthcare provider, either by uploading it back to their system or following specific submission guidelines.

Who needs to complete the Medical History Questionnaire?
The Medical History Questionnaire needs to be completed by all patients seeking eye care services. It helps healthcare providers gather essential medical and personal information to better understand a patient's health.
Is there a deadline for submitting this form?
Generally, it is recommended to submit the Medical History Questionnaire before your first appointment. Check with your healthcare provider for specific submission deadlines relevant to your situation.
How do I submit the completed questionnaire?
You can submit the completed Medical History Questionnaire by uploading it to the healthcare provider’s online portal or emailing it directly if instructed. Always confirm the submission method with your eye care clinic.
What supporting documents do I need to provide with this form?
Typically, no additional documents are required with the Medical History Questionnaire. However, if you have specific medical records, bringing them to your appointment may be beneficial.
What common mistakes should I avoid while filling out the form?
Common mistakes include leaving fields blank, providing incorrect information, or forgetting to sign the form. Double-check all entries to minimize errors before submission.
How long does it take to process the Medical History Questionnaire?
Processing time for the Medical History Questionnaire may vary by clinic. Generally, it's reviewed during your appointment or within a few days, depending on their administrative workload.
What should I do if I'm unsure how to fill out a section?
If you're unsure how to complete a section of the Medical History Questionnaire, don't hesitate to ask for assistance from clinic staff or a family member. They can provide guidance to ensure accurate information.
Related Forms






Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.