Add or replace text, adjust formatting, insert legally binding eSignatures, and send documents for signing without hopping between apps.
GA DHR 700 2011-2025 free printable template
Show details
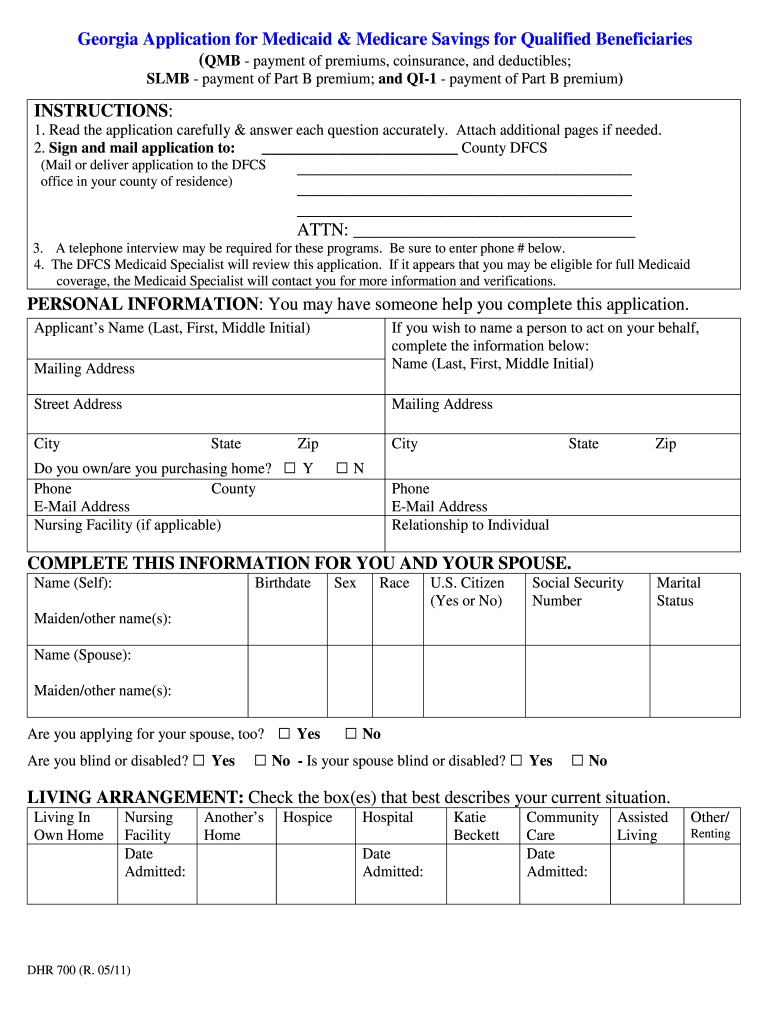
PERSONAL INFORMATION You may have someone help you complete this application. Applicant s Name Last First Middle Initial Mailing Address If you wish to name a person to act on your behalf complete the information below Name Last First Middle Initial Street Address City State Zip Do you own/are you purchasing home Phone County Nursing Facility if applicable Y N Relationship to Individual COMPLETE THIS INFORMATION FOR YOU AND YOUR SPOUSE. Name Self Birthdate Sex Race U.S. Citizen Yes or No Social...Security Number Marital Status Maiden/other name s Name Spouse Are you applying for your spouse too Are you blind or disabled Yes Yes No - Is your spouse blind or disabled Yes LIVING ARRANGEMENT Check the box es that best describes your current situation. Living In Own Home Nursing Facility Date Admitted DHR 700 R. 05/11 Another s Home Hospice Hospital Katie Beckett Community Care Assisted Other/ Renting HEALTH INSURANCE Do you have Medicare Are you enrolled in a Medicare HMO or Medicare Drug...program Does your spouse have Medicare Type of Coverage Effective Date Part A Part B Part D RX doctor Medicare Number Have you ever received SSI If so when did it end Has your spouse Do you have other health insurance If you answered yes to either of these questions please complete the following information Health Insurance Effective Policy Company Name Hospital Medicare Address and Telephone Supplement Drugs Major Medical Self Spouse Attach copies front and back of Medicare and insurance cards...if applicable. Georgia Application for Medicaid Medicare Savings for Qualified Beneficiaries QMB - payment of premiums coinsurance and deductibles SLMB - payment of Part B premium and QI-1 - payment of Part B premium INSTRUCTIONS 1. Read the application carefully answer each question accurately. Attach additional pages if needed* 2. Sign and mail application to County DFCS Mail or deliver application to the DFCS office in your county of residence ATTN 3. A telephone interview may be required for...these programs. Be sure to enter phone below. 4. The DFCS Medicaid Specialist will review this application* If it appears that you may be eligible for full Medicaid coverage the Medicaid Specialist will contact you for more information and verifications. REAL PROPERTY Do you own all or part of any real estate in which you do not live Yes No If yes please complete the following for each piece of real estate. Do not list the house or mobile home in which you live. Address Value Amount Owed Do...you or your spouse own a car truck boat camper utility trailer recreational vehicle etc* Yes No If yes please complete the following information about each vehicle. Attach additional pages if needed* Type Year Make Model RESOURCES Check all resources assets owned by you your spouse or jointly owned with someone else. Include any accounts or properties on which your name s appear. Attach additional pages if necessary. Checking account Funeral plans/ prepaid burial item Yes No Savings account...Burial plots or contracts Stocks and bonds Government bonds Trust funds Other IRA CD promissory note etc* Yes No Have you or your spouse given away any assets for less than its value Type of Resource Account/ Policy Name of Bank Insurance Company Etc* Policy Owner Insurance Company Policy Number Face Cash Value INCOME AND EARNINGS List all types of earnings and income that you and your spouse receives.
pdfFiller is not affiliated with any government organization
Fill out, sign, and share forms from a single PDF platform
Manage all your documents quickly and securely in the cloud.
Edit and sign in one place
Create professional forms
Add and customize fillable fields to tailor each form to your needs and ensure easy completion without printing and scanning.
Simplify data collection
Quickly share forms via email or a secure link, enabling anyone to complete forms online in seconds, on any device.
Manage forms centrally
Keep all your forms and templates organized in one secure, cloud-based platform, track changes easily, and export documents in any format.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
Understanding the GA DHR-2025 Form
What is the GA DHR-2025 Form
The GA DHR-2025 form is an official application used in Georgia to apply for Medicaid and Medicare savings programs. This form assists qualified beneficiaries in accessing financial support to cover medical expenses.
Eligibility Criteria for the GA DHR-2025 Form
To successfully complete the GA DHR 700 form, applicants must meet specific eligibility criteria. Typically, these criteria include being a resident of Georgia, meeting income and asset limits, and being eligible for Medicare. This ensures that assistance is provided to those who need it the most.
How to Fill the GA DHR-2025 Form
Filling out the GA DHR 700 form requires careful attention to detail. Applicants should provide accurate information, including personal details, financial information, and details about any existing health insurance. It is advisable to gather all necessary documents beforehand to facilitate a smooth application process.
Required Documents and Information
Submitting the GA DHR 700 form necessitates certain documents. Commonly required items include proof of income, Social Security numbers, Medicare card details, and any other relevant health insurance information. Having these documents ready can expedite the application process.
Submission Methods and Delivery
The completed GA DHR 700 form can be submitted through various methods, ensuring accessibility for all applicants. Submissions can be made by mail or delivered in person to the local Department of Family and Children Services (DFCS) office. It's important to check for specific submission addresses based on your county.
Best Practices for Accurate Completion
To enhance the accuracy and effectiveness of the GA DHR 700 application, applicants should double-check all entered information, use clear handwriting, and ensure that all sections of the form are completed. Seeking assistance from someone familiar with the form can also be beneficial.
Frequently Asked Questions about georgia application for medicaid and medicare form
What should I do if my application for the GA DHR 700 form is denied?
If your application is denied, you can request a review of the decision. It's important to understand the reasons for the denial and provide any additional information if necessary.
Can I apply for someone else using the GA DHR 700 form?
Yes, you can apply on behalf of someone else if you have their consent and necessary documentation to support their application.
pdfFiller scores top ratings on review platforms
This works great .... we love it ...... it made it easy to complete our 501(c)(3)app.
I have found forms through PDFfiller that I could not locate anywhere else--wonderful tool!
It's fairly intuitive, but there are some cumbersome issues related to printing--too many steps--could be simplified.
People Also Ask about online georgia 700 form for medicaid
What is QMB and SLMB?
• Qualified Medicare Beneficiary (QMB): Covers the cost of (1) Medicare. Parts A and B monthly premiums and (2) payments of coinsurance and deductible amounts for services covered under both Medicare Parts A and B. • Specified Low-Income Medicare Beneficiary (SLMB): Pays only the monthly Medicare Part B premiums.
What's the difference between QMB and SLMB?
Because the SLMB program is for people with higher incomes, SLMBs get fewer benefits than QMBs. The SLMB program pays the Medicare Part B monthly premium, but doesn't pay any Medicare deductibles or coinsurance amounts.
What is the difference between QMB and Medicaid?
Is QMB Full Medicaid? While QMB is administered by your state Medicaid agency, it's a separate program from Medicaid and provides different coverage. For example, Medicaid covers vision and dental, but QMB doesn't. Qualifying for QMB does not mean you automatically qualify for Medicaid.
Does Social Security count as income for QMB?
Does Social Security count as income for QMB? Yes, Social Security is considered income. If your monthly Social Security check exceeds $1,235 a month for an individual, you will not qualify for the Qualified Medicare Beneficiary (QMB) program in most states.
What is the difference between QMB and SLMB?
If your income is slightly too high for you to qualify for QMB benefits, you may still be eligible for another state medical assistance program: Specified Low-Income Medicare Beneficiary (SLMB). The resource limits for SLMB eligibility are the same as for a QMB, but the income limits are 20% higher.
Related pages
Related Content GA DHR 700
Related to GA DHR 700






Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.