Last updated on Mar 26, 2016
Get the free Pediatric Surgery New Patient Referral Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
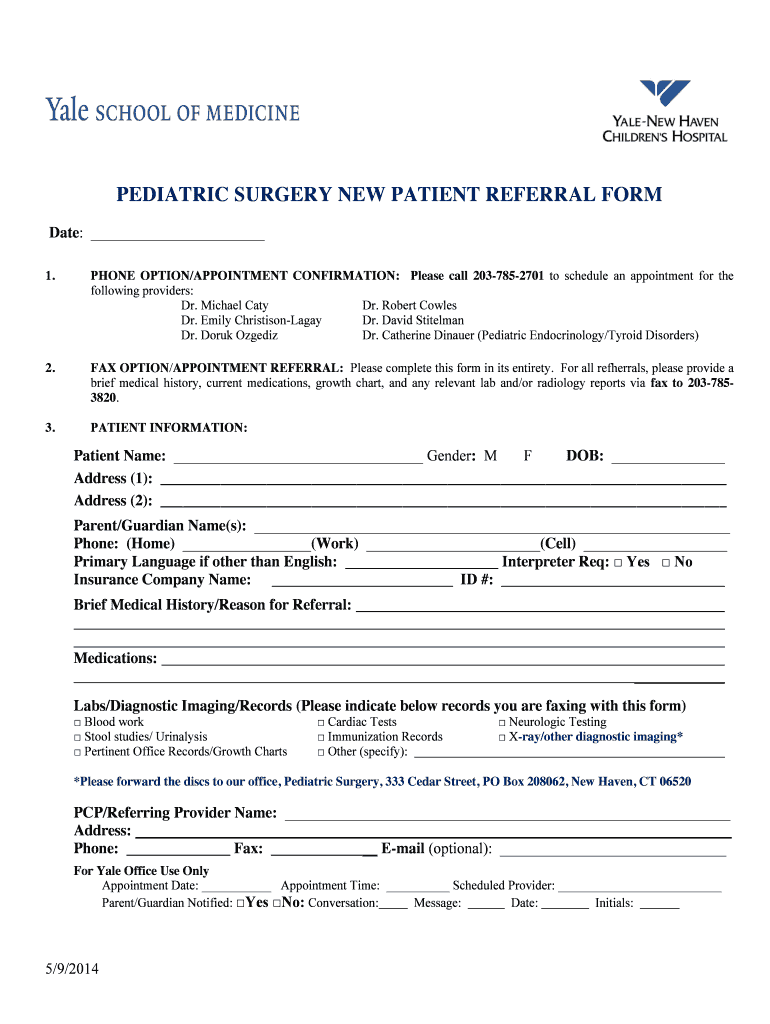
What is Pediatric Referral Form
The Pediatric Surgery New Patient Referral Form is a healthcare document used by parents or guardians to schedule pediatric surgery appointments and provide essential medical information for new patients.
pdfFiller scores top ratings on review platforms
Who needs Pediatric Referral Form?
Explore how professionals across industries use pdfFiller.

Pediatric Referral Form is needed by:
-
Parents or guardians of children needing surgery
-
Pediatricians making referrals
-
Healthcare facilities handling pediatric surgeries
-
Medical records departments reviewing patient details
-
Insurance companies for authorization purposes
Comprehensive Guide to Pediatric Referral Form
What is the Pediatric Surgery New Patient Referral Form?
The Pediatric Surgery New Patient Referral Form is a crucial tool designed to facilitate pediatric surgery appointments. Its primary function is to collect essential information that supports the pediatric surgery department in managing new patient data effectively. The form gathers details such as patient demographics, medical history, and current medications, ensuring a smooth scheduling experience for both healthcare providers and patients.
Purpose and Benefits of the Pediatric Surgery New Patient Referral Form
Accurate information plays a vital role in scheduling appointments and treatment processes. Utilizing the pediatric surgery new patient referral form benefits both patients and healthcare providers by streamlining appointment scheduling and simplifying medical record reviews. This ensures that the surgical team has the relevant information needed to plan procedures efficiently.
Key Features of the Pediatric Surgery New Patient Referral Form
The referral form includes various fillable fields, such as:
-
Patient name and gender
-
Date of birth and address
-
Parent/guardian contact information
-
Insurance details and medical history
-
Current medications and lab reports
Additionally, the form incorporates checkboxes for different types of records and requires information about the referring provider. This structure helps to capture all necessary documentation to support the referral process.
Who Should Use the Pediatric Surgery New Patient Referral Form?
The primary users of the pediatric surgery new patient referral form are parents or guardians of children who need surgical consultations. The form is applicable for various surgeries and consultations, ensuring that healthcare providers receive all pertinent information. Referring physicians play a crucial role in completing the form accurately, as this supports the overall referral process.
How to Complete the Pediatric Surgery New Patient Referral Form Online
To complete the pediatric surgery new patient referral form using pdfFiller, follow these steps:
-
Access the form through the pdfFiller platform.
-
Fill in patient demographics, including name, date of birth, and contact information.
-
Provide insurance details and parent/guardian information.
-
Complete sections related to medical history, current medications, and lab reports.
-
Review the information for accuracy before submission.
Ensuring the completeness and accuracy of the provided information is key to a successful referral process.
Submission Methods for the Pediatric Surgery New Patient Referral Form
The pediatric surgery new patient referral form can be submitted through various methods, including:
-
Faxing the completed form to the pediatric surgery department
-
Submitting the form online via pdfFiller
Be aware of potential fees or processing times associated with submission. Tracking the submission status and obtaining confirmation helps ensure the form has been received.
Security and Compliance with Pediatric Surgery New Patient Referral Form
When using pdfFiller, robust data protection measures are in place. The platform ensures compliance with HIPAA and GDPR regulations, safeguarding sensitive patient information throughout the referral process. Users can rest assured that their submitted information is handled with the utmost privacy and care.
Examples and Sample of a Completed Pediatric Surgery New Patient Referral Form
For reference, an example of a filled pediatric surgery new patient referral form can provide invaluable guidance. It highlights common pitfalls to avoid, such as missing details or incorrect information. Utilizing visual learning techniques helps clarify the submission process, ensuring all necessary information is included.
Why Choose pdfFiller for Your Pediatric Surgery New Patient Referral Form?
pdfFiller stands out for its user-friendly interface and comprehensive features, including:
-
Editing and filling capabilities
-
eSigning options for quick completion
-
Document management tools
The platform also prioritizes security, making it an ideal choice for handling sensitive healthcare forms. User satisfaction is consistently high, reflecting the effectiveness of pdfFiller in streamlining the referral process.
Take the Next Step with the Pediatric Surgery New Patient Referral Form
Utilizing pdfFiller for your pediatric surgery new patient referral form enhances efficiency and ease in the form-filling process. The platform offers additional features that support the completion and management of important documents. Timely and accurate submission of the referral form is critical to ensuring your child's healthcare needs are addressed promptly.
How to fill out the Pediatric Referral Form
-
1.Access the Pediatric Surgery New Patient Referral Form on pdfFiller by navigating to the provided link or searching for it in the pdfFiller document library.
-
2.Once the form is open, familiarize yourself with the layout, and use the toolbar to zoom in for easier reading.
-
3.Collect all necessary information before starting, including the child’s personal details, medical history, current medications, and any previous lab or imaging results.
-
4.Begin by entering the patient's full name, gender, and date of birth in the designated fields. Make sure the information is accurate and up-to-date.
-
5.Next, fill in the address section, including both the patient's address and the parent or guardian's contact information.
-
6.In the insurance information area, provide the necessary details for coverage. Ensure all fields are completed accurately to minimize processing delays.
-
7.Continue by filling out the medical history section. Include any existing health conditions, allergy details, and current medications, as this aids in the child’s medical review.
-
8.Be attentive to the checkboxes available for specific lab tests or imaging records. Select appropriate options based on previous reports.
-
9.Once all sections of the form are filled, review the completed details for any errors or missing information to ensure correctness.
-
10.After verification, save your work by clicking on the save icon, which allows you to store the form in your pdfFiller account.
-
11.Finally, choose your submission method by faxing it directly to the pediatric surgery department or downloading it for later use.

Who is eligible to use the Pediatric Surgery New Patient Referral Form?
The Pediatric Surgery New Patient Referral Form is designed for parents or guardians of children who require a referral to schedule an appointment for pediatric surgery.
What information is required to complete this form?
You will need to provide patient information, medical history, current medications, insurance details, and relevant lab or imaging records to complete the form.
How should I submit the completed form?
Once completed, the form should be faxed directly to the pediatric surgery department, or it can be downloaded and submitted based on specific instructions from your healthcare provider.
What are common mistakes to avoid when filling out the form?
Common mistakes include providing incomplete information, missing signatures, and failing to check the correct boxes for medical records. Ensure all information is accurate and complete.
Is there a deadline for submitting the referral form?
It's advisable to submit the Pediatric Surgery New Patient Referral Form as soon as possible to ensure timely scheduling of the appointment, especially if it's for a specific surgery date.
What should I do if I need assistance completing the form?
If you need help filling out the form, consult your child's pediatrician or contact the pediatric surgery department for guidance through the process.
How long does it take to process the referral once submitted?
Processing times for referrals can vary, but typically allow a few days for review before the pediatric surgery department contacts you to schedule the appointment.
Related Forms






Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.