Last updated on Mar 26, 2016
Get the free Ohio Medicaid Hospital Adjustment Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
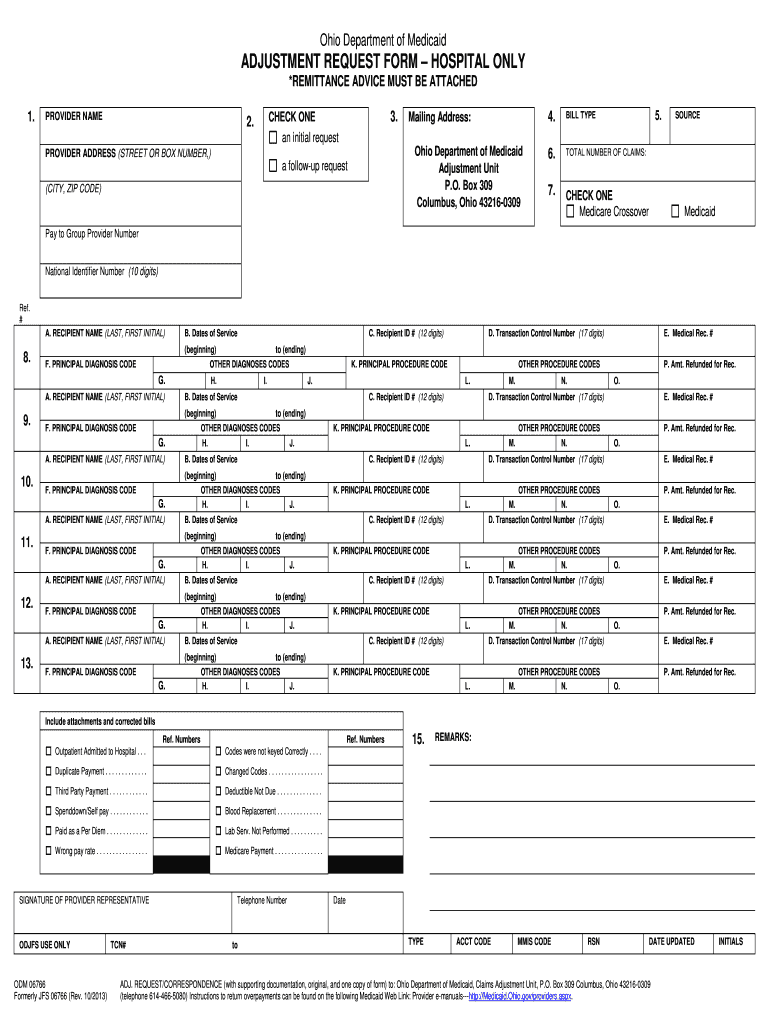
What is Ohio Medicaid Adjustment Form
The Ohio Medicaid Hospital Adjustment Request Form is a medical billing document used by healthcare providers to request adjustments to Medicaid payments for hospital services.
pdfFiller scores top ratings on review platforms
Who needs Ohio Medicaid Adjustment Form?
Explore how professionals across industries use pdfFiller.

Ohio Medicaid Adjustment Form is needed by:
-
Healthcare providers in Ohio seeking Medicaid payment adjustments
-
Billing specialists involved in hospital financing
-
Medical administrators managing Medicaid claims
-
Provider representatives responsible for compliance
-
Financial officers of healthcare facilities processing Medicaid reimbursements
Comprehensive Guide to Ohio Medicaid Adjustment Form
What is the Ohio Medicaid Hospital Adjustment Request Form?
The Ohio Medicaid Hospital Adjustment Request Form is designed for healthcare providers in Ohio to request adjustments to Medicaid payments for hospital services. This essential document establishes a standardized process for making adjustment requests, thus enhancing billing accuracy and efficiency for service providers. It is typically utilized when corrections to payment claims are necessary, making it crucial for billing departments and healthcare professionals managing Medicaid claims.
This form serves as a vital tool for healthcare providers in ensuring they receive the correct Medicaid reimbursements, ultimately affecting their operational success.
Purpose and Benefits of the Ohio Medicaid Hospital Adjustment Request Form
The Ohio Medicaid Hospital Adjustment Request Form streamlines the Medicaid billing process for healthcare providers. By utilizing this form, hospitals can effectively address billing discrepancies, which enhances overall billing accuracy. This leads to improvements in revenue cycle management, ensuring that healthcare providers are accurately compensated for their services.
The benefits include expedited payment processes and better financial management, facilitating healthier financial operations within hospitals.
Who Needs the Ohio Medicaid Hospital Adjustment Request Form?
This form is intended for healthcare providers who bill Medicaid for hospital services. Key roles that need to be involved in the completion and signing of the form include Provider Representatives. Hospitals often find themselves needing to file adjustments for various reasons, including correcting billing errors or addressing disputes related to services provided.
Understanding the target audience helps ensure that the claims process runs smoothly, ultimately benefiting both providers and patients.
Eligibility Criteria for the Ohio Medicaid Hospital Adjustment Request Form
To be eligible to utilize the Ohio Medicaid Hospital Adjustment Request Form, healthcare providers must adhere to specific criteria related to the types of services rendered and documentation. The services covered by this form must be aligned with Medicaid guidelines, and adjustments must fall within established eligibility criteria.
This clarity in eligibility helps prevent unnecessary claims rejection and streamlines the adjustment process.
How to Fill Out the Ohio Medicaid Hospital Adjustment Request Form Online
Filling out the Ohio Medicaid Hospital Adjustment Request Form online involves several specific steps:
-
Access the form on the Medicaid website or through designated platforms.
-
Input necessary information such as provider details, recipient information, and dates of service.
-
Ensure to attach required documentation, including remittance advice.
This structured approach assists healthcare providers in efficiently submitting adjustment requests and reduces the likelihood of errors.
Field-by-Field Instructions for the Ohio Medicaid Hospital Adjustment Request Form
When completing the Ohio Medicaid Hospital Adjustment Request Form, focus on the following common fields:
-
Provider Name: Clearly print the name of the healthcare provider.
-
Recipient Name: Provide the name of the patient receiving services.
-
Dates of Service: Specify the dates when services were rendered.
-
Signature of Provider Representative: Ensure that the form is signed by an authorized representative.
Each field needs to be filled out accurately to avoid processing delays.
Submission Methods and Delivery of the Ohio Medicaid Hospital Adjustment Request Form
Providers have various submission methods for the Ohio Medicaid Hospital Adjustment Request Form, including:
-
Digital submission through approved online platforms.
-
Mailing hard copies to the designated Medicaid office.
Adopting recommended practices, such as tracking submissions, enhances the likelihood of timely processing and minimizes potential issues.
What Happens After You Submit the Ohio Medicaid Hospital Adjustment Request Form?
Once the Ohio Medicaid Hospital Adjustment Request Form is submitted, it undergoes several processing steps by Medicaid. Providers can check the status of their application through specified channels, ensuring transparency in the adjustment process.
Common reasons for rejection may include incomplete forms or ineligible adjustment requests, which can be addressed through specific resubmission procedures.
How pdfFiller Supports Completing the Ohio Medicaid Hospital Adjustment Request Form
pdfFiller offers significant advantages for completing the Ohio Medicaid Hospital Adjustment Request Form. Key features include eSigning capabilities, document editing, and secure sharing options. With 256-bit encryption, pdfFiller ensures compliance with privacy regulations such as HIPAA and GDPR, giving users peace of mind while handling sensitive information.
Utilizing pdfFiller simplifies the process of managing healthcare forms effectively and securely.
Final Thoughts on Using the Ohio Medicaid Hospital Adjustment Request Form Effectively
Utilizing the Ohio Medicaid Hospital Adjustment Request Form is critical for ensuring timely and accurate Medicaid payments, and pdfFiller offers valuable support throughout the completion and submission process. Providers are encouraged to take action on their forms efficiently, supported by pdfFiller's user-friendly platform and assistance options available.
How to fill out the Ohio Medicaid Adjustment Form
-
1.Access and open the Ohio Medicaid Hospital Adjustment Request Form on pdfFiller by searching for the form name in the document search bar.
-
2.Once you locate the form, click on it to open it in the pdfFiller interface for editing.
-
3.Before you start filling the form, gather all necessary information including the provider's name, address, recipient details, and the dates of service.
-
4.Use the text fields to input the required information such as 'Provider Name', 'Recipient Name', and 'Dates of Service' directly into the designated areas of the form.
-
5.Make sure to sign the form electronically by navigating to the signature field and using the signature tool available on pdfFiller.
-
6.Review all entered information to ensure accuracy before finalizing the document. Check that totals and types of bills are correctly filled and that a remittance advice is attached.
-
7.Once satisfied with the completed form, save your changes in pdfFiller, download a copy in your preferred format, or submit the form directly to the appropriate Medicaid office using provided options.

Who is eligible to use the Ohio Medicaid Hospital Adjustment Request Form?
The form is designed for healthcare providers in Ohio who have submitted claims to Medicaid and need to adjust their payment requests due to discrepancies or issues with original claims.
What supporting documents are required when submitting this form?
When submitting the Ohio Medicaid Hospital Adjustment Request Form, ensure you attach any necessary remittance advice related to the original claim, which helps verify the adjustments being requested.
How should I submit the completed form after filling it out?
Once you have filled out and reviewed the Ohio Medicaid Hospital Adjustment Request Form, you should submit it according to your healthcare facility's procedures. This may include emailing it to the Medicaid office or sending it via postal mail.
Are there common mistakes to avoid when completing this form?
Common mistakes include failing to sign the form, providing incorrect recipient or service date details, and not attaching required supporting documents such as remittance advice, which can delay processing.
What is the expected processing time for this form?
Processing times for the Ohio Medicaid Hospital Adjustment Request Form can vary, but typically, you can expect a response within 30 days. Check with your Medicaid office for specifics.
Related Forms





Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.