Last updated on Mar 28, 2016
Get the free Ancillary Provider Data Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
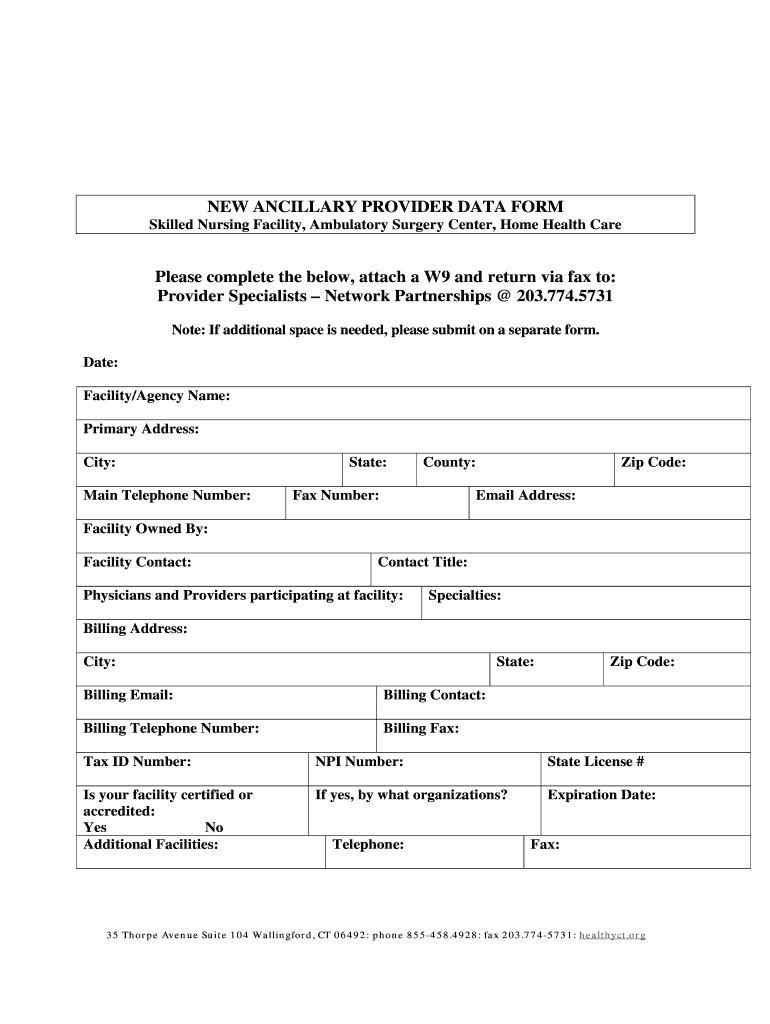
What is Provider Data Form
The Ancillary Provider Data Form is a medical billing document used by healthcare providers to submit their facility information for network partnerships.
pdfFiller scores top ratings on review platforms
Who needs Provider Data Form?
Explore how professionals across industries use pdfFiller.

Provider Data Form is needed by:
-
Skilled Nursing Facilities seeking partnership opportunities
-
Ambulatory Surgery Centers needing to provide facility information
-
Home Health Care agencies applying for network agreements
-
Healthcare Providers looking to submit billing details
-
Billing and administrative staff managing provider data
Comprehensive Guide to Provider Data Form
What is the Ancillary Provider Data Form?
The Ancillary Provider Data Form is a specialized document used by healthcare providers to submit crucial information for network partnerships. This form serves as an essential tool for establishing collaborations between various healthcare facilities, such as Skilled Nursing Facilities and Home Health Care agencies. By providing detailed information about the facility, it helps to streamline the provider network integration process.
This form requires specific data like facility name, address, and tax identification number. It is pivotal for ensuring that healthcare provider networks maintain accurate and up-to-date records about their participating specialists and facilities.
Why Use the Ancillary Provider Data Form?
Utilizing the Ancillary Provider Data Form offers several key benefits for healthcare facilities. Firstly, it simplifies and streamlines the submission process, making it more efficient for providers to join networks. Secondly, this form plays a critical role in establishing robust provider networks, ensuring that all necessary data is collected accurately and expediently.
Moreover, using this form can significantly reduce errors and improve communication among healthcare partners, fostering better relationships and operational efficiency.
Who Needs the Ancillary Provider Data Form?
The Ancillary Provider Data Form is essential for specific healthcare providers, including Skilled Nursing Facilities, Home Health Care agencies, and ambulatory surgery centers. These entities must complete the form to be eligible for inclusion in provider networks.
Typically, facilities that offer ancillary services need to fill out this form. To qualify, they must adhere to certain eligibility criteria, ensuring they meet the necessary standards to participate in network partnerships.
How to Fill Out the Ancillary Provider Data Form Online (Step-by-Step)
Completing the Ancillary Provider Data Form online involves a few simple steps:
-
Begin by entering your facility or agency name at the top of the form.
-
Fill in primary address details, including city, state, and zip code.
-
Provide contact information, including main telephone number and email address.
-
Include billing details such as the billing contact's name, phone number, and tax ID.
-
Indicate your facility's certification or accreditation status and its expiration date.
-
Double-check all information for accuracy before submission.
These steps are crucial for ensuring that the form is filled out correctly and can be processed without delays.
Common Errors and How to Avoid Them
When filling out the Ancillary Provider Data Form, several common errors often occur. These may include omissions of required fields, providing incorrect tax ID numbers, or failing to sign where necessary. Such mistakes can lead to delays in processing and complications in establishing provider networks.
To avoid these pitfalls, users should carefully review the form prior to submission. It’s helpful to have all necessary documents on hand while completing the form to ensure every detail is accurate and complete.
Required Documents and Supporting Materials
Alongside the Ancillary Provider Data Form, certain documents are necessary to complete the submission process. Key requirements may include:
-
A completed W9 form, necessary for tax purposes.
-
Documentation of certification or accreditation status.
-
Any additional licenses or certifications required by the state.
Gathering these supporting materials in advance can help streamline the process and enhance submission accuracy.
Submission Methods and Delivery
Once the Ancillary Provider Data Form is completed, several submission methods are available for sending it securely. Users can choose to fax or email the form to the designated contact provided on the form. Specify the recipient’s information correctly to ensure it is routed properly.
Being aware of the submission options can facilitate quicker processing and integration into healthcare provider networks.
What Happens After You Submit the Ancillary Provider Data Form?
After submission, the processing time for the Ancillary Provider Data Form can vary. Generally, users can expect a confirmation of receipt within a few days. It is important to keep an eye on the status of the submission, as tracking your submission helps identify any issues early.
Staying informed will contribute to a smoother experience and timely integration into the network.
Security and Compliance for Submitting Your Form
When submitting sensitive documents, security and compliance are paramount. The Ancillary Provider Data Form submission process incorporates robust security measures to protect data integrity. These may include encryption protocols and strict access controls.
Additionally, compliance with regulations such as HIPAA and GDPR is maintained rigorously, ensuring that personal and healthcare information is safeguarded throughout the submission process.
Maximize Your Ancillary Provider Data Form Experience with pdfFiller
Enhancing your experience with the Ancillary Provider Data Form is easily achievable by utilizing pdfFiller. This platform offers various features that aid in filling out, eSigning, and editing forms efficiently and securely.
With pdfFiller’s cloud-based system, users benefit from easy document management, allowing for secure storage and sharing of sensitive information without the need for lengthy downloads.
How to fill out the Provider Data Form
-
1.Access pdfFiller and search for the Ancillary Provider Data Form in the documents section or utilize the provided link.
-
2.Open the form in pdfFiller to allow for convenient editing and completion of the required fields.
-
3.Before starting to fill the form, gather all necessary information, including facility name, address, contact details, tax ID, NPI number, and certification status.
-
4.Begin by entering the 'Facility/Agency Name' at the top of the form, followed by the 'Primary Address', 'City', and 'Zip Code'.
-
5.Continue filling out the 'Main Telephone Number' and 'Email Address' in the designated fields for communication.
-
6.For billing-related information, accurately fill in sections such as 'Billing Contact', 'Billing Telephone Number', and 'Billing Fax'.
-
7.Indicate whether the facility is 'Certified or Accredited' and provide the 'Expiration Date' if applicable.
-
8.Ensure to complete any additional fields that may pertain to your facility, noting any necessary checkboxes or options.
-
9.Once all fields are completed, review the form for any errors or missing information before submission.
-
10.After confirming the accuracy, save the filled form to your personal storage on pdfFiller, ensuring it is easy to locate.
-
11.You can download the completed document in your preferred format or directly send it to the designated fax number as indicated.

Who is eligible to fill out the Ancillary Provider Data Form?
Healthcare providers such as Skilled Nursing Facilities, Ambulatory Surgery Centers, and Home Health Care agencies are eligible to complete the Ancillary Provider Data Form.
What documents are required to accompany the Ancillary Provider Data Form?
It is recommended to include a W9 form along with the Ancillary Provider Data Form to ensure all tax identification information is accurately presented.
How can I submit the Ancillary Provider Data Form once completed?
After filling out the Ancillary Provider Data Form on pdfFiller, you can submit it by faxing to the provided number as stated in the form instructions.
What information is needed to fill out the Ancillary Provider Data Form?
Collect information such as your facility name, address, contact details, tax ID, NPI number, license number, and billing details prior to completing the form.
Is there a deadline for submitting the Ancillary Provider Data Form?
While specific deadlines may vary based on partnership agreements, it is advisable to submit the Ancillary Provider Data Form as soon as your facility information is ready.
What are common mistakes to avoid when completing this form?
Ensure all fields are accurately filled without leaving blanks, double-check contact information, and avoid common errors such as incorrect tax ID numbers or NPI numbers.
How long does it take to process the Ancillary Provider Data Form?
Processing times may vary, but it typically takes a few days to a couple of weeks. Check with the organization you're submitting to for specific time frames.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.