Last updated on Mar 28, 2016
Get the free Letter of Medical Necessity Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
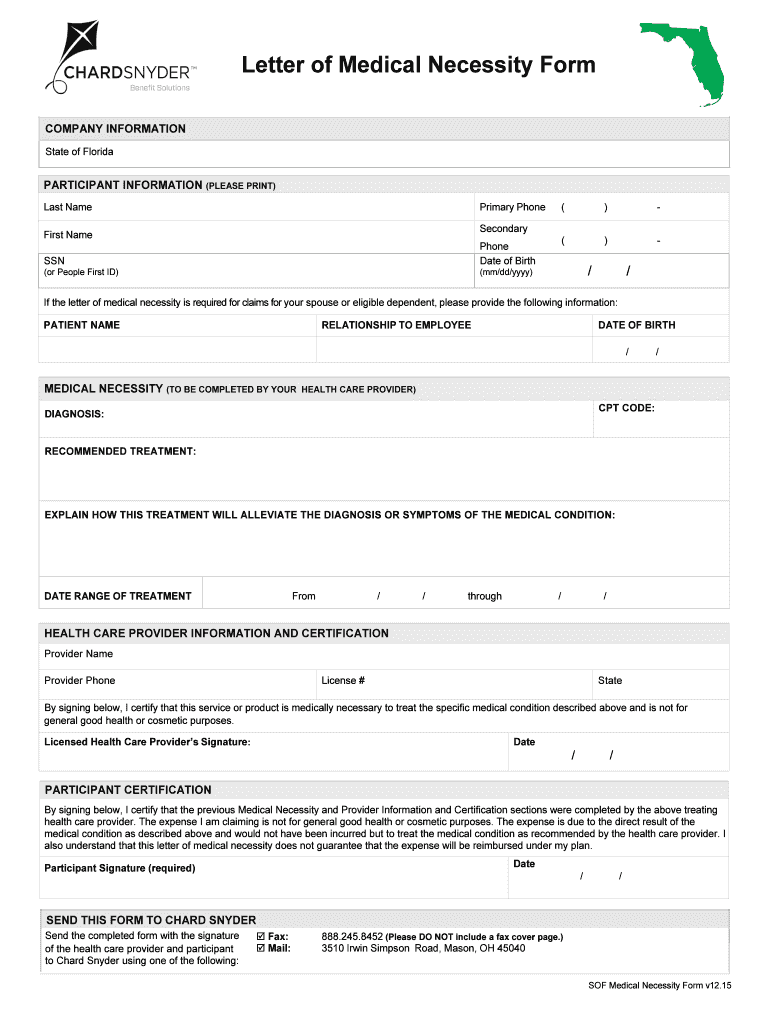
What is Medical Necessity Form
The Letter of Medical Necessity Form is a medical consent document used by healthcare providers and participants to certify the necessity of specific medical treatments for diagnosed conditions.
pdfFiller scores top ratings on review platforms
Who needs Medical Necessity Form?
Explore how professionals across industries use pdfFiller.

Medical Necessity Form is needed by:
-
Licensed health care providers certifying medical necessity
-
Participants seeking reimbursement through FSA
-
Patients requiring documented medical treatments
-
Insurance companies validating claims
-
Healthcare facilities processing treatment claims
-
Administrative staff handling medical forms
Comprehensive Guide to Medical Necessity Form
What is the Letter of Medical Necessity Form?
The Letter of Medical Necessity Form serves a critical purpose in healthcare by providing documentation that certifies specific medical treatments or products are necessary for diagnosed medical conditions. Both a Licensed Healthcare Provider and the Participant involved are required to complete this form. It includes essential fields such as 'Last Name,' 'First Name,' 'Diagnosis,' and 'Recommended Treatment' to ensure comprehensive and accurate information submission.
Purpose and Benefits of the Letter of Medical Necessity Form
This form plays a pivotal role in securing healthcare reimbursements by facilitating the certification of necessary treatments. By enabling health insurance claims for prescribed services, it greatly assists participants in obtaining reimbursement for qualified medical expenses, including Flexible Spending Account (FSA) claims. Utilizing a medical necessity form template can simplify the documentation process and ensure that all pertinent details are thoroughly captured.
Who Needs the Letter of Medical Necessity Form?
The Letter of Medical Necessity Form is essential for various stakeholders, primarily patients and healthcare providers. The roles of the Licensed Healthcare Provider involve verifying medical conditions and recommending suitable treatments. Participants, on the other hand, provide personal details and may need to present this form under specific conditions, such as when submitting claims for insurance coverage or other financial benefits.
How to Fill Out the Letter of Medical Necessity Form Online (Step-by-Step)
Completing the Letter of Medical Necessity Form online is straightforward, especially using platforms like pdfFiller. Follow these steps to ensure accuracy:
-
Start by entering your Last Name and First Name.
-
Provide the necessary details such as your SSN and Date of Birth.
-
Specify the Diagnosis related to the medical treatment.
-
Detail the Recommended Treatment planned.
-
Ensure both the healthcare provider and participant sign the form.
Taking the time to review each field thoroughly will enhance the accuracy of your submission.
Information You'll Need to Gather Before Completing the Form
Before filling out the form, collect all necessary information, including:
-
The participant's medical history relevant to the treatment.
-
Details of the recommended treatment.
-
Any supporting documents, such as previous treatment records.
A pre-filing checklist is advisable to ensure all relevant documents are prepared and ready for submission.
Common Errors and How to Avoid Them
Common mistakes when completing the Letter of Medical Necessity Form can lead to rejection of claims. To minimize these errors, consider the following tips:
-
Double-check all entries for accuracy.
-
Have another individual review the form before submission.
-
Use a review checklist to confirm that all required fields are completed.
How to Submit the Letter of Medical Necessity Form
There are various methods available for submitting the completed Letter of Medical Necessity Form, including online submission and traditional mail. Ensure that you send the form to Chard Snyder for processing. Be mindful of submission deadlines, and keep track of confirmations and any follow-up requirements after submission.
Security and Compliance for the Letter of Medical Necessity Form
Security is paramount when handling the Letter of Medical Necessity Form, as it contains sensitive personal health information. pdfFiller employs robust security measures, including 256-bit encryption, to ensure data protection. Additionally, compliance with HIPAA and GDPR safeguards the privacy of users, emphasizing the importance of protecting personal information at all times.
Examples and Templates for the Letter of Medical Necessity Form
Accessing a sample or template of the Letter of Medical Necessity Form can greatly aid in understanding how to complete it accurately. These templates are available for download on pdfFiller and demonstrate the required structure and content for the form. Utilizing a medical necessity form template makes it easier for users to provide the necessary details without overlooking any essential elements.
Experience Hassle-Free Filling of the Letter of Medical Necessity Form with pdfFiller
Using pdfFiller can significantly enhance your experience in managing the Letter of Medical Necessity Form. This cloud-based PDF editor provides convenient features for creating and editing fillable forms, as well as eSigning documents securely. The platform's compliance with privacy standards ensures that your sensitive information remains protected throughout the process.
How to fill out the Medical Necessity Form
-
1.To begin, access the pdfFiller website and search for the Letter of Medical Necessity Form using the search bar.
-
2.Once located, click on the form to open it in the pdfFiller editor interface.
-
3.Before filling out the form, gather necessary information including the participant's personal details, medical condition, and recommended treatments.
-
4.Begin with the 'Last Name' and 'First Name' fields, entering the participant's details accurately.
-
5.Next, fill in the 'SSN' and 'Date of Birth' fields, ensuring all information is correct to avoid processing delays.
-
6.Locate the 'CPT CODE' and 'DIAGNOSIS' fields. Provide accurate codes and descriptions for the medical treatment required.
-
7.In the 'RECOMMENDED TREATMENT' field, detail the suggested treatment or product that is necessary for the participant’s medical condition.
-
8.Both the healthcare provider and the participant should ensure they sign where indicated on the form.
-
9.After filling out all required fields, take a moment to review the entire form for accuracy and completeness, ensuring no fields are left blank.
-
10.Once satisfied with the completed form, save it on pdfFiller by clicking the 'Save' option, or download it directly to your device.
-
11.You may submit the form electronically through pdfFiller or print it out for physical submission to Chard Snyder for FSA reimbursement processing.

Who is eligible to use the Letter of Medical Necessity Form?
The form is designated for licensed health care providers and the participants receiving treatment, ensuring both parties sign to validate the medical necessity.
What information do I need before filling out the form?
Gather the participant's personal information, including their name, SSN, date of birth, diagnosis details, recommended treatment, and any applicable medical codes.
How do I submit the Letter of Medical Necessity Form?
After completing the form, you can submit it electronically through pdfFiller or print and send it physically to Chard Snyder for reimbursement claiming.
What common mistakes should I avoid when completing the form?
Ensure all fields are completed accurately, particularly diagnosis and treatment details. Avoid leaving any required fields blank to prevent delays in processing.
How long does it take to process the form once submitted?
Processing times can vary. Typically, expect a few business days, but always check directly with Chard Snyder for specific timelines.
Is there a fee associated with submitting this form?
Generally, there are no fees for utilizing the form itself, but check with your healthcare provider or the administrative office for any possible fees associated with processing.
What should I do if I encounter issues filling out the form on pdfFiller?
If issues arise while using pdfFiller, check their support resources or contact their customer service for assistance with the form completion process.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.