Last updated on Mar 28, 2016

Get the free Client Medical History and Physician Statement
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
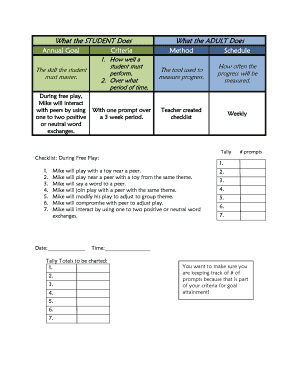
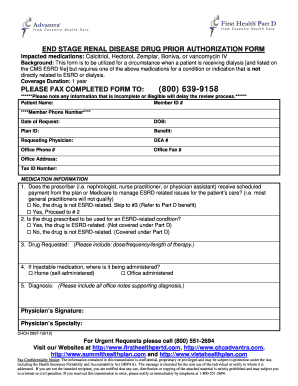
What is Medical History Form
The Client Medical History and Physician Statement is a medical document used by physicians to evaluate a client's medical history and assess their ability to participate in supervised equine activities.
pdfFiller scores top ratings on review platforms
Who needs Medical History Form?
Explore how professionals across industries use pdfFiller.

Medical History Form is needed by:
-
Physicians assessing patients for equine activities
-
Patients undergoing medical evaluations for special needs
-
Medical offices requiring documentation for client history
-
Equine activity organizers needing medical confirmation
-
Any healthcare providers managing patient mobility evaluations
Comprehensive Guide to Medical History Form
What is the Client Medical History and Physician Statement?
The Client Medical History and Physician Statement is a crucial form utilized to capture an individual's medical history. This form comprises several essential components, including a detailed medical history section, a thorough physician evaluation, and a mobility assessment. It is significant for the physician's signature to verify the authenticity of the information provided and to affirm the physician's medical assessment.
Purpose and Benefits of the Client Medical History and Physician Statement
This form plays a vital role in documenting a client's medical history, particularly when participating in equine activities. It not only streamlines the assessment process for healthcare providers but also offers clients a comprehensive overview of their health status. Accurate documentation is essential for effective patient care, ensuring all medical conditions are taken into account during evaluations.
Key Features of the Client Medical History and Physician Statement
The form includes various sections designed for thorough completion, covering areas such as:
-
Diagnoses
-
Medications
-
Surgeries
-
Special needs
Users will find a combination of checkboxes and blank fields, allowing for detailed input. Additionally, there are explicit instructions provided for physicians to ensure the form is completed correctly and signed appropriately.
Who Needs the Client Medical History and Physician Statement?
The target audience for this form includes physicians who assess patients for specific activities, especially those involving equine participation. Patients with particular medical conditions that may impact their ability to engage in such activities will also benefit from this evaluation. Situations such as events or facility usage may necessitate the completion of this form.
How to Fill Out the Client Medical History and Physician Statement Online (Step-by-Step)
To complete the form online, follow these straightforward steps:
-
Access the form using pdfFiller.
-
Fill in personal details in the designated fields.
-
Provide comprehensive medical history, including diagnoses and medications.
-
Complete the mobility assessment section carefully.
-
Ensure all required fields are filled out and read the instructions for physician completion.
Pay special attention to highlighted areas that may require extra detail to ensure accuracy and completeness.
Review and Validation Checklist for the Client Medical History and Physician Statement
Before submitting the form, it is essential to review it for common errors. Use the following checklist to validate your document:
-
Confirm the physician has signed the document.
-
Ensure all fields are completed, with no blanks where information is required.
-
Review for any discrepancies or inaccuracies in the information provided.
This thorough review process is critical for compliance and accurate representation of the patient’s health.
How to Sign the Client Medical History and Physician Statement
Signing this document can be done digitally or through traditional means. For digital signing using pdfFiller, follow these steps:
-
Open the document in pdfFiller.
-
Select the eSigning option.
-
Follow the prompts to add your digital signature securely.
It is essential to ensure that the signing process adheres to secure methods to protect sensitive information.
Submitting the Client Medical History and Physician Statement
The completed form can be submitted in several ways:
-
Online submission through pdfFiller.
-
Physical mailing to the designated facility or physician.
Be sure to check for any state-specific requirements that may apply and consider tracking options to confirm receipt after submission.
Security and Compliance for Handling the Client Medical History and Physician Statement
Ensuring the security of sensitive information is paramount. pdfFiller follows strict data protection standards, including compliance with HIPAA and GDPR. Key measures include:
-
Utilization of 256-bit encryption for data protection.
-
Commitment to secure storage and handling practices.
These measures provide users with confidence that their medical documents are safely managed.
Experience Efficient Document Management with pdfFiller
pdfFiller offers comprehensive capabilities that streamline document processing, including editing, eSigning, and sharing. Users are encouraged to utilize pdfFiller not only for the Client Medical History and Physician Statement but also for various other document needs. The platform is designed with a user-friendly interface and provides cloud-based convenience for efficient form management.
How to fill out the Medical History Form
-
1.Access the Client Medical History and Physician Statement form on pdfFiller. Search for the form using the search bar or browse through the healthcare forms category.
-
2.Open the form by clicking on its title. The pdfFiller interface will display the form in an editable format.
-
3.Before filling out the form, gather relevant medical records, including past diagnoses, surgeries, medications, and any special needs information that you'll need to input.
-
4.Begin by completing the client's basic information such as name, date of birth, and contact details in the designated fields.
-
5.Fill out the sections regarding medical history, including any relevant diagnoses and treatments. Use the checkboxes provided to indicate any special conditions.
-
6.If there are areas pertaining to mobility and the use of assistive devices, ensure to detail the client's capabilities and necessary adaptations.
-
7.Once you have filled out all required fields, review each entry carefully for accuracy and completeness. Confirm that all medical history information is correct.
-
8.After making sure everything is accurate, the physician must sign the form. Look for the signature field, and apply an electronic signature or print for physical signing.
-
9.Finalize the document by saving your progress. Use the 'Save' or 'Download' options to store an electronic copy securely.
-
10.To submit the form, check if you've selected the correct submission method. You can typically email it directly from pdfFiller or download it for physical submission.

Who is eligible to complete the Client Medical History and Physician Statement form?
The form is specifically designed for physicians who need to document a client's medical history and assess their ability to engage in equine activities.
Is there a deadline for submitting this form?
While there may not be a strict deadline for submitting the form, it is best to complete it as soon as possible to ensure timely evaluations and participation in equine activities.
How can I submit the completed form?
You can submit the completed form by either emailing it directly from pdfFiller or downloading it and then mailing it or submitting it in person, depending on the requirements of the activity organizers.
What supporting documents do I need to provide with the form?
You may need to provide medical records that support any claims made in the form, including documentation of diagnoses or treatments relevant to the client's medical history.
What common mistakes should I avoid when filling out the form?
Be sure to fill out all required fields completely and accurately. Avoid leaving any blanks and double-check for any medical terms that may need clarification.
How long does it take to process the Client Medical History and Physician Statement form?
Processing times can vary depending on the physician's schedule, but typically, it should take no longer than a few business days for the evaluation to be completed.
What information is required in the medical history section?
The medical history section requires details such as previous diagnoses, surgeries, medications, and any special needs that may affect the client's ability to participate in equine activities.
Related Forms




Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.