Last updated on Mar 28, 2016
Get the free Dental Provider Information Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
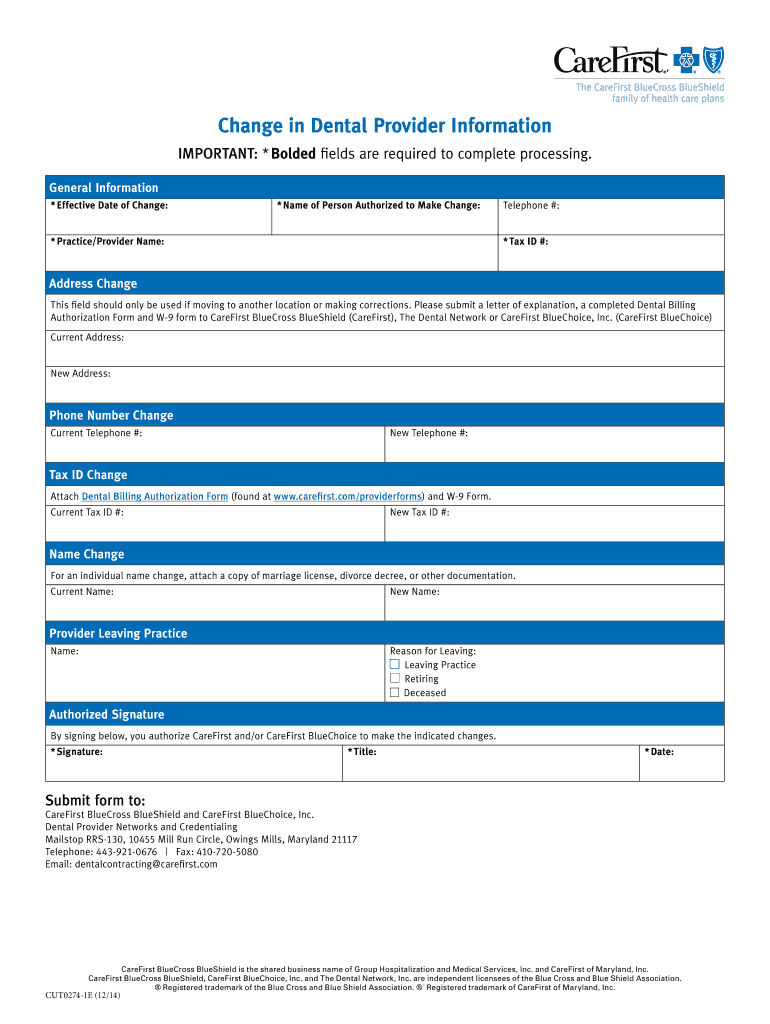
What is Dental Provider Change
The Dental Provider Information Change Form is a medical document used by dental providers to update their information with CareFirst BlueCross BlueShield.
pdfFiller scores top ratings on review platforms
Who needs Dental Provider Change?
Explore how professionals across industries use pdfFiller.

Dental Provider Change is needed by:
-
Dental Providers requiring address updates
-
Practices changing tax ID information
-
Providers updating phone numbers
-
Authorized personnel handling billing questions
-
Dental networks in Maryland
-
Practitioners retiring or transferring practice location
Comprehensive Guide to Dental Provider Change
What is the Dental Provider Information Change Form?
The Dental Provider Information Change Form is a critical document for dental providers looking to update their details with CareFirst. This form serves several key purposes, including updating important information such as address, phone number, tax ID, and name. Alongside the form, providers must submit specific documentation, which includes a letter of explanation, a completed Dental Billing Authorization Form, and a W-9 form where applicable.
Why You Need the Dental Provider Information Change Form
Timely updates through the Dental Provider Information Change Form are essential to ensure accurate billing and effective patient care. Outdated information can lead to complications in processing claims and may even affect patient services. Moreover, complying with CareFirst’s requirements is crucial; failing to file the form or doing so late can result in administrative hurdles and potential pitfalls regarding provider status.
Who Should Use the Dental Provider Information Change Form?
The target audience for the Dental Provider Information Change Form includes any dental provider authorized to make changes on behalf of their entity. The role of the "Authorized Person" is vital as only they can submit the necessary updates. This form is applicable for various dental providers, including independent dentists and dental group practices, particularly when changes in address, name, or tax ID are necessary.
Key Features of the Dental Provider Information Change Form
This form contains several essential components that ensure the accuracy and completeness of submitted information. Key sections include:
-
Effective date of the change
-
Name of the person authorized to make the change
-
Signature requirements
The document also includes blank fields and checkboxes, necessitating accuracy in entries to avoid processing delays.
How to Fill Out the Dental Provider Information Change Form Online
To fill out the Dental Provider Information Change Form online using pdfFiller, follow these steps:
-
Access the form through pdfFiller's platform.
-
Edit specific fields as needed, using the provided digital tools.
-
Follow field-by-field guidance to complete each section accurately.
-
Utilize options for digital signatures to streamline the process.
Using pdfFiller enhances the filing experience and ensures all necessary elements are in place.
Required Documents and Supporting Materials
Submitting the Dental Provider Information Change Form requires accompanying documentation, such as:
-
A letter of explanation detailing the changes
-
A completed Dental Billing Authorization Form
-
A W-9 form for tax ID updates
Accurate documentation plays a significant role in expediting the processing of the form, so it is essential to ensure that all required materials are included with your submission.
Submission Process for the Dental Provider Information Change Form
Once the Dental Provider Information Change Form is completed, there are several methods to submit it:
-
Email the completed form to CareFirst.
-
Mail the physical form to the designated address provided by CareFirst.
It is crucial to receive confirmation of submission and to track the status post-submission to avoid any potential setbacks.
Common Mistakes to Avoid When Submitting the Dental Provider Information Change Form
To ensure smooth processing, avoid the following common pitfalls when submitting the Dental Provider Information Change Form:
-
Leaving fields incomplete, particularly those marked with asterisks.
-
Neglecting to provide necessary signatures.
-
Filing without validating all provided information.
Utilizing pdfFiller tools can help mitigate these errors by allowing you to review the document thoroughly before submission.
How pdfFiller Can Help with the Dental Provider Information Change Form
pdfFiller offers numerous advantages for completing the Dental Provider Information Change Form efficiently. Key features include:
-
Editing capabilities for precise information input.
-
eSigning options that simplify the signature process.
-
Cloud storage for secure document handling and easy retrieval.
Using pdfFiller ensures the safe management of sensitive information while providing a hassle-free experience for users.
Next Steps After Submitting the Dental Provider Information Change Form
Following the submission of the form, providers should take certain follow-up actions:
-
Check the status of your submission through the designated channels.
-
Be prepared to address any issues if the submission is rejected.
-
Maintain organized records of all documents and communications.
Adhering to these steps ensures better compliance and readiness for any future updates or resubmissions.
How to fill out the Dental Provider Change
-
1.Access the Dental Provider Information Change Form by visiting pdfFiller and searching for the form name.
-
2.Once located, click on the form to open it in pdfFiller's interactive interface.
-
3.Review the complete form structure to familiarize yourself with the required sections and inputs needed.
-
4.Before starting, gather necessary information such as your current contact details, tax ID, and any documentation like W-9 forms or letters of explanation.
-
5.Fill in each required field, paying attention to asterisks that denote mandatory information.
-
6.Complete sections such as 'Effective Date of Change' and 'Name of Person Authorized to Make Change' in the designated areas.
-
7.Use the tools provided by pdfFiller to add text or check boxes as needed for your changes.
-
8.Once all fields are filled, review the form carefully to ensure all information is accurate and complete.
-
9.Utilize pdfFiller’s features to check for any missing required fields or errors before finalizing the form.
-
10.After review, save your changes in pdfFiller, allowing for easy retrieval and editing if needed.
-
11.Download the completed form as a PDF or submit it directly through the platform following the submission guidelines provided by CareFirst.

Who is eligible to submit the Dental Provider Information Change Form?
The form is primarily for dental providers and authorized personnel who need to update their information with CareFirst BlueCross BlueShield.
Are there any deadlines for submitting this form?
While specific deadlines may vary, it's crucial to submit the form promptly to ensure your provider information is current and prevent billing issues.
What methods can I use to submit the completed form?
You can submit the completed form through pdfFiller directly or follow CareFirst's submission guidelines for physical mail or secure online submission methods.
What supporting documents do I need to include with the form?
You need to include a completed Dental Billing Authorization Form, W-9 for tax ID changes, and a letter of explanation if applicable.
What common mistakes should I avoid when filling out this form?
Ensure all required fields are filled out completely, double-check accuracy of information, and avoid submitting without necessary supporting documents.
How long does it usually take to process this form?
Processing times can vary, but typically allow several weeks for updates to be reflected in CareFirst's systems after submission.
Are there any fees associated with submitting this form?
Generally, there are no fees for submitting the Dental Provider Information Change Form itself, but ensure compliance with any related billing authorization procedures.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.