Last updated on Mar 28, 2016
Get the free Pharmacy Prior Authorization Form for Tecfidera
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
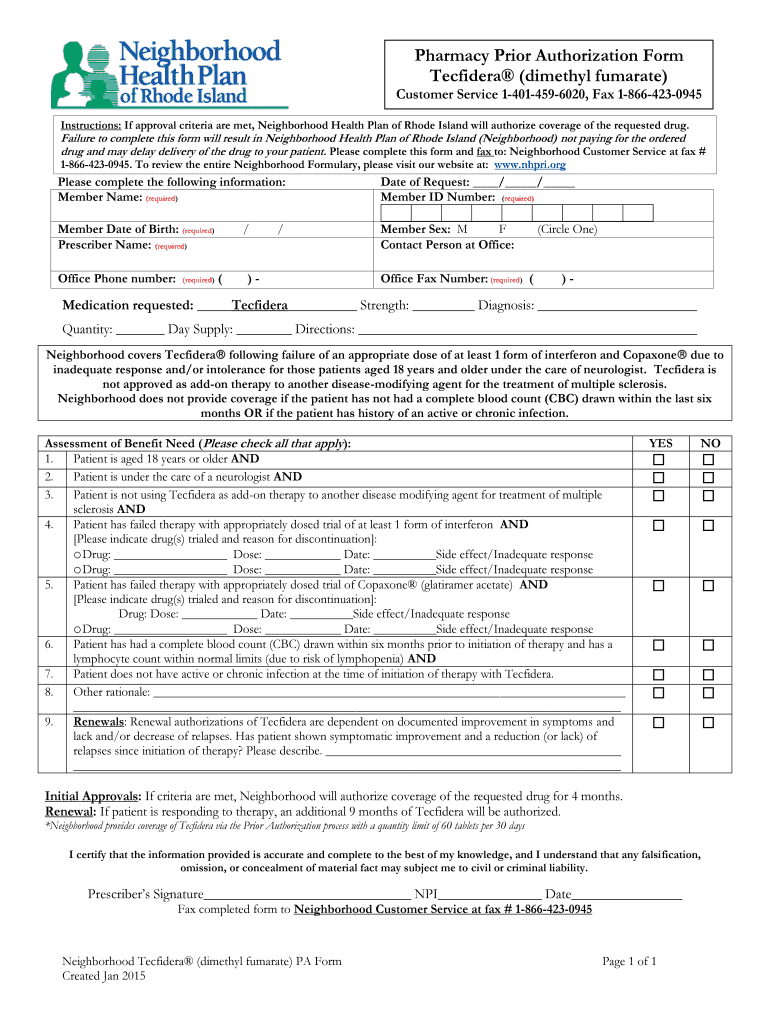
What is Tecfidera PA Form
The Pharmacy Prior Authorization Form for Tecfidera is a medical consent document used by prescribers to request approval for Tecfidera under Neighborhood Health Plan of Rhode Island.
pdfFiller scores top ratings on review platforms
Who needs Tecfidera PA Form?
Explore how professionals across industries use pdfFiller.

Tecfidera PA Form is needed by:
-
Healthcare providers prescribing Tecfidera
-
Administrative staff managing prior authorization requests
-
Patients seeking medication coverage through insurance
-
Pharmacists processing medication prescriptions
-
Insurance companies verifying medication requests
Comprehensive Guide to Tecfidera PA Form
What is the Pharmacy Prior Authorization Form for Tecfidera?
The Pharmacy Prior Authorization Form for Tecfidera is a vital document that facilitates the request for medication coverage through the Neighborhood Health Plan of Rhode Island. This form ensures that patients requiring Tecfidera (dimethyl fumarate) can effectively communicate their medical needs to their insurance provider.
By completing this form, healthcare providers can streamline the process of obtaining authorization for this essential multiple sclerosis medication. The form serves as an official request for the insurance company to cover the costs associated with Tecfidera, making it an integral part of the healthcare process.
Purpose and Benefits of the Pharmacy Prior Authorization Form for Tecfidera
The Pharmacy Prior Authorization Form is crucial for patients as it outlines the necessary steps for securing insurance coverage for Tecfidera. It helps patients by ensuring that their prescribed medication is accessible without undue delay.
-
This form minimizes the risk of coverage denial by providing comprehensive information required by insurance providers.
-
It facilitates a more efficient approval process, allowing prescribers to gather needed documentation succinctly.
-
Patients benefit from expedited access to necessary treatments, improving overall health outcomes.
Eligibility Criteria for the Pharmacy Prior Authorization Form for Tecfidera
To utilize the Pharmacy Prior Authorization Form for Tecfidera, patients must meet specific eligibility criteria set by Neighborhood Health Plan. These criteria typically involve the patient's diagnosis and treatment history related to multiple sclerosis.
Key considerations include:
-
Patients must have a confirmed diagnosis of multiple sclerosis.
-
There may be age restrictions that apply to the authorization process.
Required Information for Completing the Pharmacy Prior Authorization Form for Tecfidera
Completing the Pharmacy Prior Authorization Form requires detailed patient-specific information to ensure a smooth submission process. Providers will need to gather the following:
-
Patient's full name, date of birth, and insurance information.
-
Diagnosis and relevant medical history, including previous treatments for multiple sclerosis.
-
Prescriber’s details, including licensing information and signature.
How to Fill Out the Pharmacy Prior Authorization Form for Tecfidera Online (Step-by-Step)
Filling out the Pharmacy Prior Authorization Form online through pdfFiller simplifies the process. Follow this step-by-step guide for a successful submission:
-
Access the form on the pdfFiller platform.
-
Enter the required patient information in the designated fields.
-
Provide details about the patient’s medical history and previous treatments.
-
Have the prescriber sign the form electronically.
-
Review the completed form for accuracy before submission.
Submission Methods for the Pharmacy Prior Authorization Form for Tecfidera
After filling out the Pharmacy Prior Authorization Form, it is crucial to submit it correctly for processing. There are several methods to ensure the form reaches the appropriate department:
-
The primary method is to fax the completed form directly to Neighborhood Health Plan.
-
Ensure that the fax number is correct to avoid delays in processing.
-
Keep a copy of the submitted form and fax confirmation for your records.
What Happens After You Submit the Pharmacy Prior Authorization Form for Tecfidera?
Once the Pharmacy Prior Authorization Form is submitted, patients and prescribers should be prepared for the next steps. Approval or denial timelines can vary significantly:
-
Typically, approval decisions are communicated within a few days to a week.
-
Patients and prescribers can track the status of their submission through customer service or portals provided by Neighborhood Health Plan.
Common Issues with the Pharmacy Prior Authorization Form for Tecfidera and How to Resolve Them
While submitting the Pharmacy Prior Authorization Form, issues can arise that may delay the approval process. Common problems include:
-
Incomplete or inaccurate information can lead to rejection. Review all entries before submission.
-
Missing prescriber signatures must be addressed promptly to avoid resubmission.
To resolve these issues, it's essential to communicate with the prescriber and review the form thoroughly for necessary corrections prior to resubmission.
Why Choose pdfFiller for the Pharmacy Prior Authorization Form for Tecfidera?
pdfFiller simplifies the process of completing the Pharmacy Prior Authorization Form for Tecfidera with its robust features. Users can enjoy:
-
Easy editing and filling capabilities for streamlining form completion.
-
Enhanced security features to protect sensitive patient information.
-
Options for eSigning and document management, which minimize paperwork and physical storage needs.
Start Using pdfFiller to Simplify Your Pharmacy Prior Authorization Form for Tecfidera Today!
To effectively manage your Pharmacy Prior Authorization Form for Tecfidera, consider utilizing pdfFiller's cloud-based platform. With strong security measures in place, handling sensitive health information becomes a seamless experience.
Engage with pdfFiller today to start filling out your forms efficiently and securely.
How to fill out the Tecfidera PA Form
-
1.To access the Pharmacy Prior Authorization Form for Tecfidera, visit pdfFiller's website and search for the form name.
-
2.Once you locate the form, click on it to open the document in the pdfFiller interface.
-
3.Before filling out the form, gather all necessary patient information, including diagnosis details, medication dosage, and history of previous treatments.
-
4.Begin by entering the patient's information in the designated fields, ensuring accuracy for effective processing.
-
5.Next, fill in the prescriber's details, confirming that all provided information aligns with your professional registration.
-
6.Complete the medication section by specifying Tecfidera, noting any required dosage and frequency.
-
7.Utilize checkboxes to indicate the patient's health conditions and previous treatments as directed.
-
8.After filling all fields, carefully review the information to prevent errors that may delay processing.
-
9.Ensure that the prescriber signs where indicated, as a signature is mandatory for form validation.
-
10.Once finalized, utilize the pdfFiller options to save the completed form to your device or submit it electronically.
-
11.If necessary, download a copy for your records before faxing or submitting the form to Neighborhood Health Plan as required.

Who is eligible to use the Pharmacy Prior Authorization Form for Tecfidera?
The form is designed for use by healthcare providers prescribing Tecfidera in Rhode Island, as well as their administrative staff to facilitate medication coverage approval.
What supporting documents are required for submission?
Typically, you need to include detailed patient information, a medical history relevant to the prescription, and any prior treatment documentation to accompany the Pharmacy Prior Authorization Form.
How do I submit the completed form?
After completing and signing the form, fax it directly to Neighborhood Health Plan as specified in their submission guidelines to ensure timely processing.
What are common mistakes to avoid when filling out this form?
Avoid leaving fields blank, double-check the accuracy of patient and prescriber information, and confirm that the prescriber's signature is present to prevent delays in authorization.
What is the processing time for the prior authorization request?
Processing times may vary, but typically, you can expect a response within a few business days after submission. It's best to follow up if you do not receive confirmation.
Are there any fees associated with submitting this form?
Generally, there are no fees specifically tied to the submission of the Pharmacy Prior Authorization Form itself, but check with Neighborhood Health Plan for any applicable costs.
What specific patient information do I need to gather before filling out the form?
You should collect the patient's demographic information, diagnosis details, medication dosage, and any relevant history of previous treatments before starting the form.
Related Forms



Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.