Hospital Forms 8850134 2005-2026 free printable template
Show details
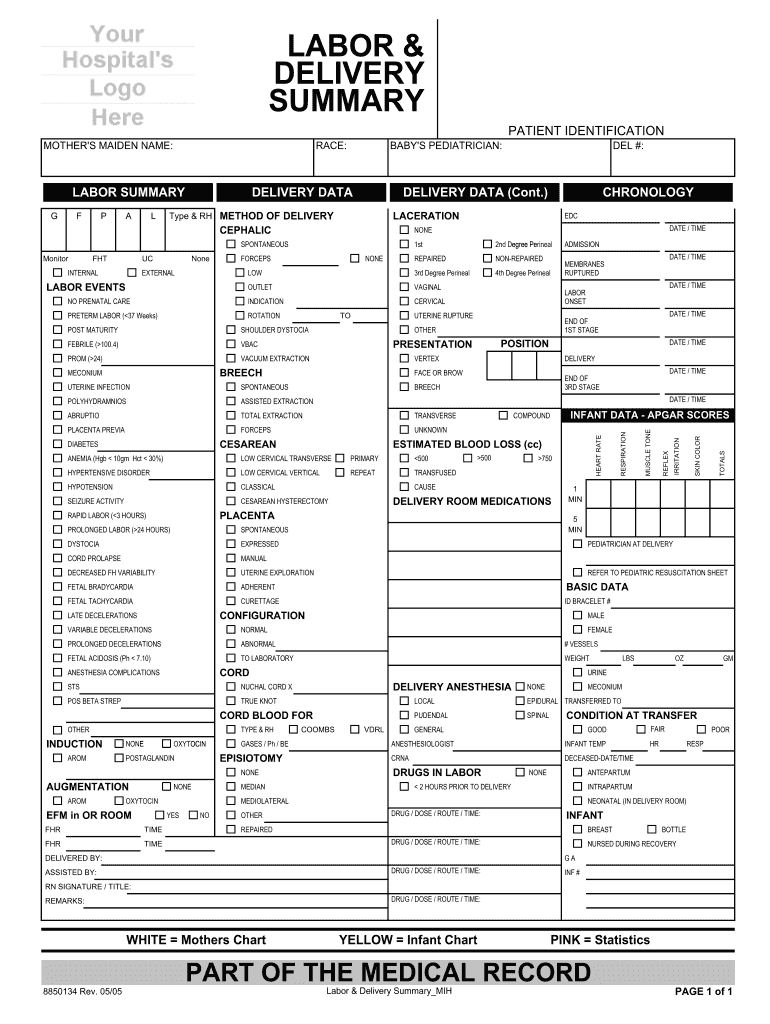
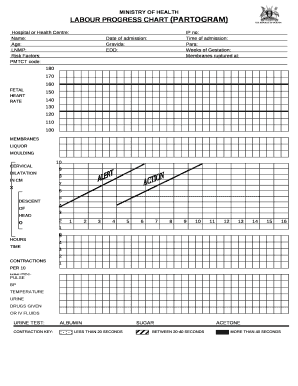
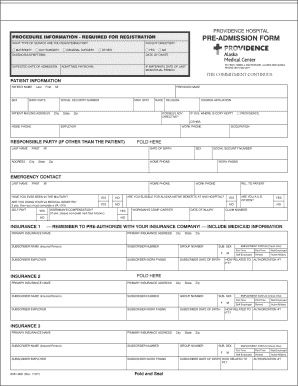
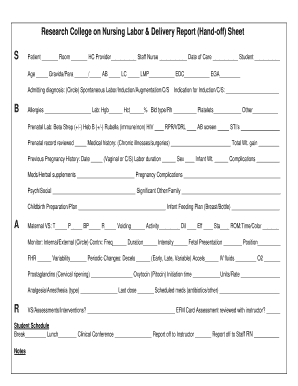
This document serves as a comprehensive summary of a patient's labor and delivery process, including details on methods of delivery, complications, maternal and infant data, and postoperative information.
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign labor and delivery charting examples form
Edit your blank partograph template form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your labor and delivery report sheet pdf form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit printable partograph pdf online



Use the instructions below to start using our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit printable partograph form. Add and change text, add new objects, move pages, add watermarks and page numbers, and more. Then click Done when you're done editing and go to the Documents tab to merge or split the file. If you want to lock or unlock the file, click the lock or unlock button.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
With pdfFiller, it's always easy to work with documents.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out labor and delivery admission questions form
How to fill out Hospital Forms 8850134
01
Gather necessary personal information, including your full name, date of birth, and contact information.
02
Provide your insurance details, including the name of your insurance provider and policy number.
03
Fill out your medical history, including any pre-existing conditions, allergies, and current medications.
04
Indicate the reason for your visit to the hospital.
05
Review the consent section and sign where required, ensuring you understand what you are consenting to.
06
Submit the completed form to the hospital's admissions desk or designated department.
Who needs Hospital Forms 8850134?
01
Patients seeking medical treatment or services at the hospital.
02
Individuals applying for admission or undergoing evaluations in the hospital.
03
Those needing to update their personal or insurance information with the hospital.
Fill
labor and delivery terms and abbreviations pdf
: Try Risk Free
People Also Ask about
How do I contact the US Department of Labor?
You may call 833-LCO-INFO (833-526-4636), or visit the office nearest you – search by alphabetical listing of cities, locations, and communities.
What are the rules around FMLA?
In order to be eligible to take leave under the FMLA, an employee must (1) work for a covered employer, (2) work 1,250 hours during the 12 months prior to the start of leave, (3) work at a location where 50 or more employees work at that location or within 75 miles of it, and (4) have worked for the employer for 12
What does FMLA stand for?
The Family and Medical Leave Act (FMLA) provides certain employees with up to 12 weeks of unpaid, job-protected leave per year.
What does the US Department of Labor do?
Our Mission To foster, promote, and develop the welfare of the wage earners, job seekers, and retirees of the United States; improve working conditions; advance opportunities for profitable employment; and assure work-related benefits and rights.
What is the FMLA in Nebraska?
FAMILY AND MEDICAL LEAVE ACT (FMLA) OF 1993 FMLA requires the State of Nebraska to provide up to 12 weeks of unpaid, job protected leave to “eligible” employees for certain family and medical reasons.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I get Hospital Forms 8850134?
With pdfFiller, an all-in-one online tool for professional document management, it's easy to fill out documents. Over 25 million fillable forms are available on our website, and you can find the Hospital Forms 8850134 in a matter of seconds. Open it right away and start making it your own with help from advanced editing tools.
How do I complete Hospital Forms 8850134 on an iOS device?
Make sure you get and install the pdfFiller iOS app. Next, open the app and log in or set up an account to use all of the solution's editing tools. If you want to open your Hospital Forms 8850134, you can upload it from your device or cloud storage, or you can type the document's URL into the box on the right. After you fill in all of the required fields in the document and eSign it, if that is required, you can save or share it with other people.
How do I edit Hospital Forms 8850134 on an Android device?
The pdfFiller app for Android allows you to edit PDF files like Hospital Forms 8850134. Mobile document editing, signing, and sending. Install the app to ease document management anywhere.
What is Hospital Forms 8850134?
Hospital Forms 8850134 is a specific document used by hospitals to report certain healthcare data, typically related to patient care or billing information.
Who is required to file Hospital Forms 8850134?
Hospitals and healthcare providers that fall under specific regulatory authorities or funding requirements are typically required to file Hospital Forms 8850134.
How to fill out Hospital Forms 8850134?
To fill out Hospital Forms 8850134, the required data must be collected, ensuring all sections are completed accurately according to the instructions provided with the form.
What is the purpose of Hospital Forms 8850134?
The purpose of Hospital Forms 8850134 is to collect and report data that is crucial for healthcare analytics, compliance purposes, and improving patient care services.
What information must be reported on Hospital Forms 8850134?
Information reported on Hospital Forms 8850134 typically includes patient demographics, treatment details, outcomes, and billing codes as required by regulatory standards.
Fill out your Hospital Forms 8850134 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Hospital Forms 8850134 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
