Last updated on Apr 1, 2016
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medical History Form
The Patient Medical History Form is a medical document used by healthcare providers to collect detailed medical information from patients.
pdfFiller scores top ratings on review platforms
Who needs Medical History Form?
Explore how professionals across industries use pdfFiller.

Medical History Form is needed by:
-
Patients needing to update their medical information
-
Healthcare providers requiring patient history for care
-
Medical offices for patient intake processing
-
Insurance companies assessing patient coverage
-
Research institutions conducting health studies
Comprehensive Guide to Medical History Form
What is the Patient Medical History Form?
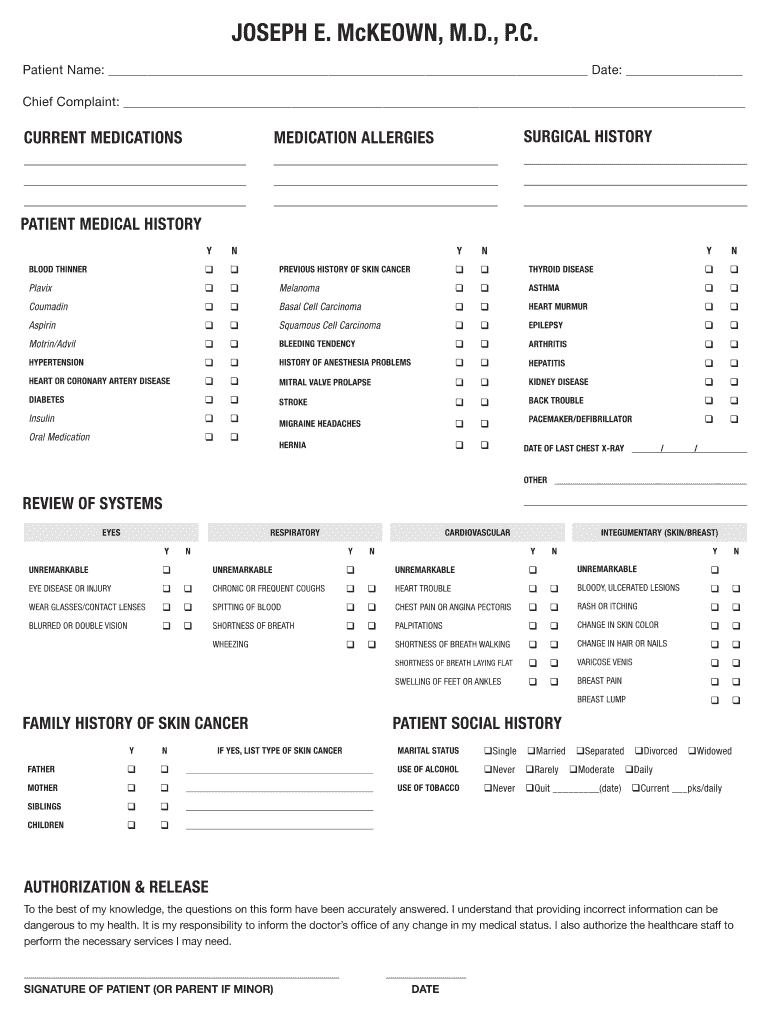
The Patient Medical History Form is a critical document in healthcare, designed to capture essential medical information about patients. This form plays a significant role for healthcare providers, allowing them to gather comprehensive data necessary for effective treatment and diagnosis. Typical information collected includes the patient's medical history, current medications, allergies, and any prior surgeries.
Healthcare providers rely on this patient medical history form to ensure they have a thorough understanding of a patient's health background, which is instrumental in providing quality care.
Purpose and Benefits of the Patient Medical History Form
The patient medical history form serves several essential purposes. It simplifies the patient intake process by providing a structured method for patients to present their medical information. This comprehensive collection of data aids in achieving accurate diagnoses and tailored treatment plans.
Moreover, having a complete medical history enhances communication between patients and healthcare providers, significantly improving the quality of care. This medical history template proves invaluable in any clinical setting where accurate patient information is crucial.
Key Features of the Patient Medical History Form
This form contains several key features that facilitate both patient and healthcare provider engagement. It includes essential sections such as patient details, chief complaints, current medications, and allergies.
-
Checkboxes for quick and easy completion of medical conditions
-
Clearly defined fields for personal and health history
-
Signature requirement for authorization and information release
These features ensure that crucial information is captured efficiently during the patient registration process.
Who Needs the Patient Medical History Form?
The target audience for the Patient Medical History Form includes new patients as well as existing patients who need to update their medical information. This document is essential across various healthcare settings, including clinics, hospitals, and specialist practices.
It is imperative that anyone visiting a healthcare provider for the first time, or requiring updates on their health status, completes this form to facilitate optimal care.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
Completing the Patient Medical History Form online is a straightforward process. Follow these steps to ensure accurate submission:
-
Access the form via pdfFiller.
-
Fill out your personal details in the designated fields.
-
Provide comprehensive information regarding your medical history.
-
Indicate any known allergies in the relevant section.
-
Review all entries for accuracy before submitting.
This step-by-step guide ensures that you efficiently fill out the medical history template, leading to a smoother intake process.
How to Sign the Patient Medical History Form
Signing the Patient Medical History Form is a crucial step for its validation. Patients can choose between digital and wet signatures, depending on their preferences and circumstances.
For those opting to eSign using pdfFiller, specific instructions guide you through the signing process, ensuring that your signature is properly captured and legally recognized. This signature is essential for the form's validity, confirming your consent to the terms within the document.
Submission Methods for the Patient Medical History Form
Once completed, there are various methods for submitting the Patient Medical History Form. Digital submission is available through pdfFiller, allowing for quick and efficient processing.
-
Mail options for those preferring traditional methods
-
In-person submission at the healthcare provider’s office
After submission, patients can confirm and track their form to ensure it has been received properly, enhancing peace of mind regarding their medical information.
Security and Compliance of the Patient Medical History Form
Data security and compliance are paramount when dealing with sensitive medical information. pdfFiller employs robust security measures, including encryption, to protect patient data. This adherence to HIPAA and GDPR ensures that patient information is handled with the utmost care.
Users can feel reassured knowing that their information remains private and secure throughout the process of completing and submitting the Patient Medical History Form.
Benefits of Using pdfFiller for Your Patient Medical History Form
Utilizing pdfFiller for your Patient Medical History Form offers numerous advantages. The platform provides an intuitive online environment for form creation, editing, and eSigning. It integrates a comprehensive document management suite aimed at making healthcare form processes as seamless as possible.
By choosing pdfFiller, users can take advantage of its diverse capabilities, ensuring a hassle-free experience in managing healthcare forms effectively.
Get Started with Your Patient Medical History Form Today!
Accessing and completing your Patient Medical History Form using pdfFiller is simple. Follow the easy steps outlined to ensure you provide accurate medical information, which is crucial for your healthcare journey.
Remember, precise details enhance the quality of care you receive. With the support and resources available through pdfFiller, starting your healthcare documentation has never been easier.
How to fill out the Medical History Form
-
1.Access the Patient Medical History Form on pdfFiller by visiting the website and using the search bar to locate the form.
-
2.Open the form by selecting it from your search results. Ensure you are logged into your pdfFiller account.
-
3.Familiarize yourself with the pdfFiller interface. Scroll through the sections of the form to see where information is required.
-
4.Collect necessary information such as personal details, medical conditions, and medication history before starting to fill out the form.
-
5.Begin filling in your personal details, ensuring accuracy in entering your name, address, and contact information.
-
6.Proceed to check off any allergies, current medications, and chief complaints from the provided checkboxes.
-
7.Fill in the sections regarding your surgical history, family history, and any other relevant medical details.
-
8.Review each section once completed to confirm that all information is accurate and thorough.
-
9.Use the 'Save' feature to keep a copy of your progress, or 'Preview' to see how it looks before finalizing.
-
10.Once all fields are completed and reviewed, sign the form electronically where indicated.
-
11.After signing, download the completed form or submit it directly through pdfFiller’s submission options.

Who needs to fill out the Patient Medical History Form?
Patients who are visiting a healthcare provider for the first time or updating their medical records are required to fill out this form.
Is there a deadline for submitting the Patient Medical History Form?
There’s typically no formal deadline, but it’s best to submit the form as early as possible, preferably before your medical appointment.
Can I edit the form after I've filled it out?
Yes, you can make edits to the form anytime before you finalize and submit it on pdfFiller. Make sure to review before submitting.
What happens if I make a mistake filling out the form?
If you make an error, you can easily correct it while you’re still in edit mode. Review your entries carefully before saving or submitting.
Do I need to notarize the Patient Medical History Form?
No, notarization is not required for the Patient Medical History Form. It only requires the patient's signature for authorization.
How will my information be used after I submit the form?
Your information will be used solely by the healthcare provider for medical assessment and care planning, following strict privacy regulations.







Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.