Last updated on Apr 2, 2016

Get the free Medical Questionnaire Supplement to Application
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medical Questionnaire
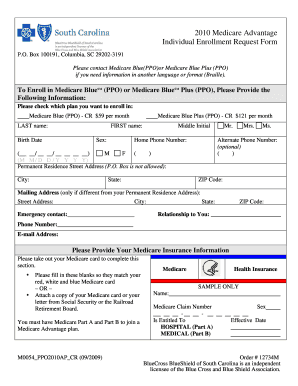
The Medical Questionnaire Supplement to Application is a medical history document used by individuals applying for insurance to provide their health information and consent for testing.
pdfFiller scores top ratings on review platforms
Who needs Medical Questionnaire?
Explore how professionals across industries use pdfFiller.

Medical Questionnaire is needed by:
-
Individuals applying for health insurance
-
Insurance agents processing applications
-
Healthcare providers requesting patient information
-
Insurance underwriters assessing risk
-
Legal representatives for insured parties
-
Family members assisting in application
Comprehensive Guide to Medical Questionnaire
What is the Medical Questionnaire Supplement to Application?
The Medical Questionnaire Supplement is a crucial document in the insurance application process. It serves to collect essential medical history from individuals seeking insurance coverage. Providing accurate medical information in this questionnaire is vital as it affects coverage decisions and premium rates. In this context, the medical history form plays a pivotal role in helping insurance providers assess risks accurately.
Purpose and Benefits of the Medical Questionnaire Supplement
The primary purpose of the medical questionnaire is to gather comprehensive health-related information necessary for underwriting insurance policies. Both applicants and insurance providers benefit from this process. For applicants, it ensures that they receive appropriate coverage based on their health needs, while insurers utilize the information to make informed decisions about risk assessment and premium calculations.
Key Features of the Medical Questionnaire Supplement to Application
-
Personal information section for identifying the applicant.
-
Medical history sections covering previous health conditions and treatments.
-
Consent sections for HIV testing and sharing results.
-
Fillable fields that guide applicants on necessary disclosures.
-
Instructions included to clarify the completion process.
Who Needs to Fill Out the Medical Questionnaire Supplement?
Individuals applying for health insurance, referred to as the proposed insured, are required to complete the medical questionnaire supplement. This form is utilized specifically in the context of an application for health insurance coverage, ensuring that insurers have a comprehensive understanding of the applicant's health status.
How to Fill Out the Medical Questionnaire Supplement Online
To efficiently fill out the medical questionnaire online via pdfFiller, follow these steps:
-
Access the form on pdfFiller’s platform.
-
Gather all necessary information, including personal medical history and family health history.
-
Begin filling out the form by entering personal details in the specified fields.
-
Review any specific instructions provided in the form to ensure accuracy.
-
Finally, submit the completed form according to the provided guidelines.
Field-by-Field Instructions for Completing the Form
Completing the medical questionnaire supplement requires attention to detail. Here are some key sections and examples:
-
Name: Provide your full legal name as it appears on identification.
-
Date of Birth: Format as month/day/year (e.g., 01/01/1990).
-
Signature: Sign your name at the designated area to confirm accuracy and consent.
-
Medical Treatments: List all treatments received, including dates and providers.
Submitting the Medical Questionnaire Supplement to Application
Once the medical questionnaire supplement has been completed, several methods are available for submission. Applicants can scan and email the document, upload it through an online portal, or submit it by mail to the insurer's address. It is essential to check for any state-specific requirements that may affect submission methods.
What Happens After Submission?
After submitting the medical questionnaire supplement, applicants typically receive confirmation of their submission. Tracking the status of the application may be possible through the insurer's online system or direct inquiry. If any issues arise, such as rejections, applicants should be prepared to provide additional information or clarifications as requested by the insurance provider.
Security and Compliance When Using the Medical Questionnaire Supplement
Users can feel confident about the security of their sensitive information when filling out the medical questionnaire supplement. Comprehensive security measures, including 256-bit encryption, are in place, ensuring compliance with regulations such as HIPAA and GDPR. This commitment to privacy and data protection helps safeguard personal health data throughout the process.
Utilizing pdfFiller for Your Medical Questionnaire Supplement Needs
pdfFiller offers robust features to enhance the process of creating, filling, and signing the medical questionnaire supplement. Users can take advantage of the cloud-based platform for convenience and ease of access. Capabilities include editing, eSigning, and sharing, making it a comprehensive solution for health insurance-related forms.
How to fill out the Medical Questionnaire
-
1.Access the Medical Questionnaire Supplement to Application on pdfFiller by searching for the form title in the search bar.
-
2.Open the form by selecting it from the search results; this will load it in the pdfFiller editing interface.
-
3.Before starting, gather necessary information such as personal identification details, medical history, and family medical background.
-
4.Begin filling in your information by clicking on the designated fields; use the text box to input your name, date of birth, and other personal details.
-
5.Follow the prompts for medical history, ensuring to answer all questions accurately; use checkboxes where applicable to provide quick responses.
-
6.Provide consent for HIV antibody testing by signing in the appropriate section, ensuring that your signature matches the name and birth date provided.
-
7.After completing all sections, carefully review your responses for accuracy and completeness; make corrections if needed.
-
8.Finalize the form by following pdfFiller’s instructions to save your changes; consider downloading a copy for your records.
-
9.Submit your completed form via the options available in pdfFiller, which typically include email, direct submission to an insurer, or downloading for postal submission.

Who is eligible to fill out this medical questionnaire?
This medical questionnaire is intended for individuals applying for insurance coverage, specifically those who are designated as the proposed insured party on the application.
What information do I need before completing the form?
Before completing the form, gather your personal identification information, detailed medical history, details about past medical treatments, and any known family medical history.
How do I submit the completed form?
Once you have completed the form on pdfFiller, you can submit it through options provided, such as emailing it to your insurance agent or downloading it for postal submission.
Are there any deadlines for submitting this questionnaire?
Deadlines for submission typically align with your insurance application process; it’s best to complete and submit the form as soon as possible to avoid delays in processing your application.
What common mistakes should I avoid when filling out the form?
To avoid mistakes, ensure that all fields are filled out accurately, your signature aligns with the name provided, and that you do not leave any required sections blank.
How long will it take to process my application after submitting the form?
Processing times can vary by insurer, but it generally takes a few days to weeks; it’s advisable to check with your insurance provider for specific timelines.
Do I need to notarize this form?
No, this Medical Questionnaire Supplement does not require notarization, but it does require the signature of the proposed insured individual for validation.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.