Last updated on Apr 2, 2016
Get the free Primary Care Network Referral Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is PCN Referral Form
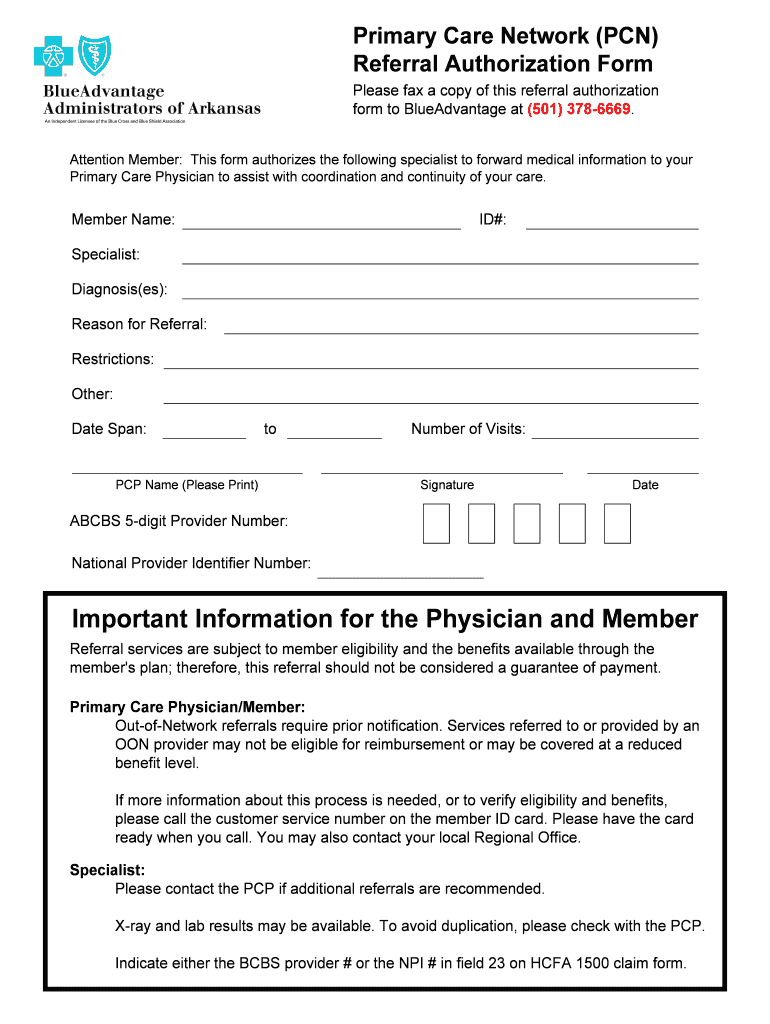
The Primary Care Network Referral Authorization Form is a healthcare document used by members to authorize a specialist to share medical information with a Primary Care Physician for coordinated care.
pdfFiller scores top ratings on review platforms
Who needs PCN Referral Form?
Explore how professionals across industries use pdfFiller.

PCN Referral Form is needed by:
-
Primary Care Physicians
-
Members seeking specialist care
-
Specialists providing referral services
-
Healthcare administrators managing patient referrals
-
Insurance providers requiring referral documentation
-
Patients needing continuity of care
Comprehensive Guide to PCN Referral Form
What is the Primary Care Network Referral Authorization Form?
The Primary Care Network Referral Authorization Form is essential for authorizing specialists to share medical information with Primary Care Physicians. This form streamlines communication, ensuring that both specialists and primary care physicians are aligned in their treatment approaches. By facilitating clear and concise information flow, it enhances the coordination of patient care.
Purpose and Benefits of the Primary Care Network Referral Authorization Form
This form is vital in coordinating patient care as it establishes a formal method for referrals. When properly utilized, the PCN referral form helps improve care continuity, allowing healthcare providers to track patient history effectively. Physicians benefit from having complete information at hand, while patients experience a smoother transition between different healthcare services.
Key Features of the Primary Care Network Referral Authorization Form
The form consists of several key sections that include:
-
Member Name
-
ID#
-
Specialist details
-
Diagnosis
-
Reason for Referral
-
Restrictions
-
Date Span
-
Number of Visits
-
PCP Name
-
Signature and Date
Additionally, security measures are implemented to protect sensitive information, ensuring compliance with healthcare regulations.
Who Needs the Primary Care Network Referral Authorization Form?
Essential roles in completing the form include the Primary Care Physician, who must sign the document; the Member, whose information is needed; and the Specialist, who will provide the referral. Newly referred patients can especially benefit from this structured approach, as it clarifies expectations and procedures for their healthcare journey.
How to Fill Out the Primary Care Network Referral Authorization Form Online (Step-by-Step)
Filling out the form using pdfFiller is straightforward:
-
Access the form through pdfFiller.
-
Begin with the Member's Name and ID#.
-
Enter the Specialist’s details and relevant diagnosis.
-
Select the Reason for Referral and any restrictions.
-
Include the Date Span and Number of Visits expected.
-
Provide the PCP Name, and ensure all sections are accurately filled.
-
Sign and date the form.
Be mindful of common mistakes such as incomplete sections or incorrect ID numbers to ensure smooth processing.
Common Errors and How to Avoid Them
When filling out the Primary Care Network Referral Authorization Form, some common errors include:
-
Missing Member Name or ID#
-
Incomplete Specialist details
-
Leaving out the Reason for Referral
-
Incorrectly filling in date ranges
To validate your entries, review each section carefully before submission. Double-checking all information can prevent delays in processing.
Submission Methods and Delivery for the Referral Authorization Form
Several methods exist for submitting the completed form, including electronic submission via pdfFiller and traditional mail. Be aware of any deadlines for submission and the expected processing times to ensure timely follow-up.
What Happens After You Submit the Primary Care Network Referral Authorization Form?
Once submitted, the next steps include tracking the form's acceptance or rejection. Users can follow up with the Primary Care Physician or the Specialist to confirm the status. Addressing any issues promptly will facilitate a smoother coordination of care.
Why Choose pdfFiller for Your Primary Care Network Referral Authorization Form
pdfFiller offers secure eSigning and efficient document management capabilities, making it an ideal platform for handling the Primary Care Network Referral Authorization Form. With its user-friendly interface, even those unfamiliar with digital forms will find it easy to navigate, ensuring a seamless experience in form completion.
Start Using the Primary Care Network Referral Authorization Form with pdfFiller Today!
Utilize pdfFiller's comprehensive services for a streamlined process in completing your healthcare referral form. The platform prioritizes security and ease of use, ensuring your sensitive information is managed appropriately.
How to fill out the PCN Referral Form
-
1.Begin by accessing the Primary Care Network Referral Authorization Form on pdfFiller. You can find it by searching for the form name in the pdfFiller search bar.
-
2.Once the form is open, navigate through the fillable fields using your mouse or keyboard. You can click directly on each required field to begin entering your information.
-
3.Before filling out the form, ensure you have all necessary details at hand. This includes the Member's name, ID number, Specialist's details, diagnosis, and the reason for the referral.
-
4.Fill in each section of the form, starting with the Member Name and ID#. Continue with the Specialist's information, including their name and contact number.
-
5.In the Diagnosis and Reason for Referral fields, provide clear and concise details relevant to your condition and the need for specialist care.
-
6.If there are any Restrictions or Other notes, fill these out as directed. Determine the Date Span and Number of Visits required for the specialist's services.
-
7.Make sure to include the Primary Care Physician's name before signing and dating the form. Ensure accurate completion of the ABCBS 5-digit Provider Number and National Provider Identifier Number if applicable.
-
8.After filling in all fields, review the form for accuracy and completeness. Check for missing information or errors before finalizing your submission.
-
9.Once satisfied, save your work by using the 'Save' option. You can download the filled form or use the 'Submit' option to send the form directly through pdfFiller, adhering to any guidelines provided.

Who is eligible to use the Primary Care Network Referral Authorization Form?
The form is designed for members seeking to authorize a specialist to forward their medical information to their Primary Care Physician. It is important that the member consults their PCP regarding this process.
What information do I need to complete the form?
Before starting, gather essential details such as your name, ID number, the specialist's name, diagnosis, reason for referral, and contact information. Ensure you have all necessary information to complete each section accurately.
How do I submit the completed form?
After filling in the form, you can submit it through pdfFiller by selecting the submission option available. Alternatively, you may download and print the form to submit it manually to your Primary Care Physician or the specialist.
Are there any deadlines for submitting the referral form?
While specific deadlines may vary, it is recommended to submit the form as soon as possible to avoid delays in receiving care from the specialist. Consult your insurance provider for any time-sensitive requirements.
What common mistakes should I avoid when filling out the form?
Ensure all required fields are completed accurately, particularly your ID number and the specialist’s contact information. Double-check the spelling of names and dates to avoid processing delays.
How long does it take to process the referral once submitted?
Processing times can vary based on the specialist and insurance provider. Generally, you should expect to receive confirmation within a few business days. Always follow up if you have not heard back.
What should I do if my referral needs to be updated?
If there are changes needed, contact your Primary Care Physician or the specialist directly. You may need to submit a new form if the changes are significant or require additional authorization.
Related Forms







Get the latest insights from our blog

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.