Last updated on Apr 3, 2016
Get the free Patient's Request for Medical Payment
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
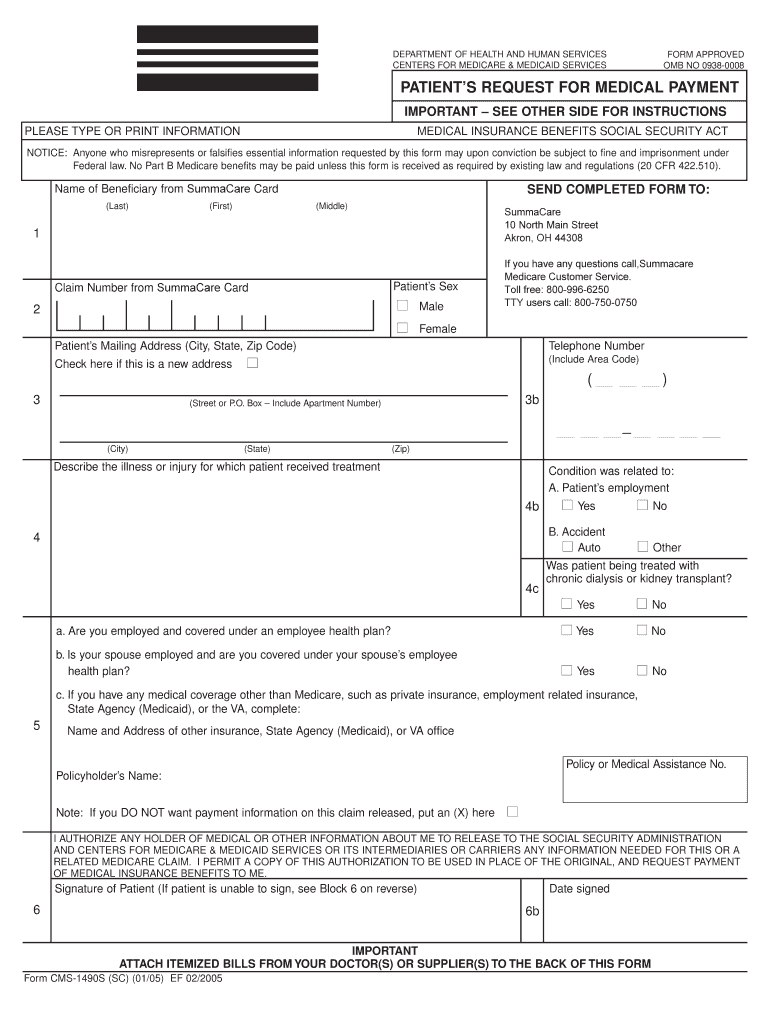
What is Medical Payment Request
The Patient's Request for Medical Payment is a healthcare form used by patients to submit a claim for Medicare benefits.
pdfFiller scores top ratings on review platforms
Who needs Medical Payment Request?
Explore how professionals across industries use pdfFiller.

Medical Payment Request is needed by:
-
Patients seeking to claim Medicare benefits
-
Caregivers assisting patients with medical claims
-
Healthcare providers submitting claims on behalf of patients
-
Insurance agents helping clients understand claims processes
-
Billing departments within medical facilities
Comprehensive Guide to Medical Payment Request
What is the Patient's Request for Medical Payment?
The Patient's Request for Medical Payment is a crucial form enabling users to submit Medicare claims. This form plays a vital role in facilitating the process of receiving benefits related to medical expenses. To complete this form, patients are required to provide personal information and relevant accompanying documentation, ensuring a smooth submission of their medicare claim form.
Purpose and Benefits of the Patient's Request for Medical Payment
Filing the Patient's Request for Medical Payment is essential for patients looking to secure their Medicare benefits. By correctly using this medicare benefit form, individuals can avoid delays and ensure that their claims are processed efficiently. The timely submission of this health insurance claim form aids in enhancing the chances of receiving the coverage that patients deserve.
Key Features of the Patient's Request for Medical Payment
This form is designed for ease of use, featuring multiple fillable fields to streamline the submission process. Key sections of the form include:
-
Name of Beneficiary
-
Patient’s Mailing Address
-
Patient’s Sex
-
Signature of Patient
These elements highlight the fillable nature of the form, making it user-friendly for those completing their summacare claim form or health insurance claim form.
Who Needs the Patient's Request for Medical Payment?
The Patient's Request for Medical Payment should be filed by individuals who have incurred medical expenses that fall under Medicare. This includes a variety of cases such as:
-
Patients undergoing outpatient procedures
-
Individuals seeking reimbursement for hospital stays
-
Those requiring claims for therapy services
Understanding the profile of those needing to file this patient medical payment request can assist in improving the claims processing experience.
How to Fill Out the Patient's Request for Medical Payment Online (Step-by-Step)
Filling out the Patient's Request for Medical Payment online can be simplified with the following step-by-step instructions:
-
Access the online form and begin with entering the Name of Beneficiary.
-
Provide the Patient’s Mailing Address accurately.
-
Complete the field labeled Patient’s Sex.
-
Review the information to ensure accuracy before submission.
These steps help ensure that essential details required for processing the medicare claim form are included, aiding in the swift handling of the patient medical payment request.
Common Errors and How to Avoid Them
To ensure accuracy in submissions, it is crucial to be aware of common mistakes made when filling out the form. Typical issues include:
-
Missing personal information
-
Failing to provide signed documentation
Before submission, reviewing the form can prevent errors and ensure that the health insurance claim form is accurately completed.
Where and How to Submit the Patient's Request for Medical Payment
Submitting the Patient's Request for Medical Payment can be done through various methods. Patients can choose to:
-
Mail the completed form to the designated Medicare address.
-
Submit the form through an online portal, if available.
It is important to accompany the form with required documentation, such as an itemized bill, to facilitate the processing of the summacare claim form or medicare claim form.
What Happens After You Submit Your Patient's Request for Medical Payment?
Upon submission of the Patient's Request for Medical Payment, patients can expect a timeline for processing the claim and receiving payment. Users can track the status of their claim through the Medicare system, allowing them to stay informed on the progress and outcomes.
Security and Compliance When Using the Patient's Request for Medical Payment
When handling the Patient's Request for Medical Payment form, pdfFiller ensures the security of sensitive information with robust measures. Key aspects of security include:
-
256-bit encryption for document protection
-
Compliance with HIPAA and GDPR regulations
This approach reassures users regarding privacy while using the health insurance claim form.
Streamline Your Medical Payment Requests with pdfFiller
Utilizing pdfFiller for the Patient's Request for Medical Payment offers numerous advantages. Key benefits include the ease of filling out the form online and enhanced efficiency in the submission process. Additionally, pdfFiller provides a secure platform that supports users through various document management tasks related to their forms.
How to fill out the Medical Payment Request
-
1.Access pdfFiller and log in to your account.
-
2.In the search bar, type 'Patient's Request for Medical Payment' and select the correct form from the search results.
-
3.Open the form in the pdfFiller editor.
-
4.Begin by entering the patient's full name in the 'Name of Beneficiary' field.
-
5.Next, fill in the 'Patient’s Mailing Address' to ensure accurate correspondence.
-
6.Select the patient's sex from the options provided.
-
7.To indicate consent, electronically sign the form in the designated 'Signature of Patient' field.
-
8.Ensure you gather all necessary information, including details about the illness or injury, as well as any other insurance coverage.
-
9.If needed, refer to the itemized bill from the doctor or supplier to complete the form accurately.
-
10.Review all entered information to confirm its accuracy and completeness.
-
11.If any discrepancies or missing information exist, correct them before moving forward.
-
12.Once satisfied with the form, click on the save option to store it.
-
13.To download a copy for your records, select the download option in pdfFiller.
-
14.Finally, submit the form as instructed by your healthcare provider or insurance company, ensuring that all required documents are attached.

Who is eligible to submit the Patient's Request for Medical Payment?
Any patient who has incurred medical expenses and holds Medicare benefits can submit this form to claim medical payments. It is essential that the patient is the one to sign the form.
What documents are required when submitting the form?
Along with the Patient's Request for Medical Payment form, an itemized bill from the healthcare provider must be submitted. Additionally, information regarding any other insurance coverage should be included.
Is there a deadline for submitting the claim?
Medicare guidelines typically require claims to be submitted within one calendar year from the date of service. Timely submission is essential to ensure payment processing.
How do I submit the Patient's Request for Medical Payment form?
You can submit the completed form and supporting documents to your Medicare Contractor. Depending on your plan, this may involve mail or electronic submission methods.
What common mistakes should I avoid when completing the form?
Common mistakes include incomplete fields, missing signatures, and failing to attach required documentation. Always double-check all entries to ensure accuracy.
How long does it take to process the claim after submission?
Processing times can vary but typically take 30 to 90 days. You should receive a notification from Medicare regarding any updates or actions needed after submission.
Can I complete the form online?
Yes, the Patient's Request for Medical Payment form can be completed online using platforms like pdfFiller, which allows for digital filling and signing.
Related Forms




Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.