Last updated on Apr 3, 2016
Get the free 2016 Benefits Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Benefits Change Form
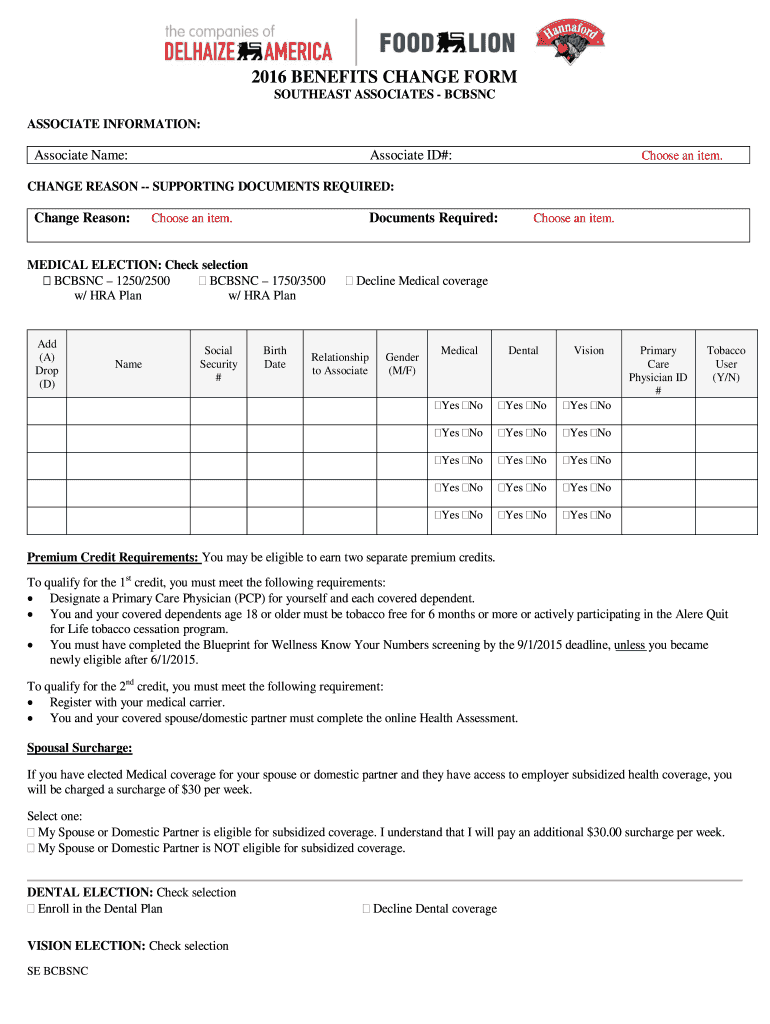
The 2016 Benefits Change Form is a Benefits Enrollment Form used by associates of Southeast Associates - BCBSNC to modify their health and life insurance benefits.
pdfFiller scores top ratings on review platforms
Who needs Benefits Change Form?
Explore how professionals across industries use pdfFiller.

Benefits Change Form is needed by:
-
Southeast Associates employees seeking to change benefits
-
HR personnel managing employee benefits
-
Life insurance beneficiaries needing to update information
-
Associates enrolling in medical, dental, and vision coverage
-
Payroll departments processing benefit changes
Comprehensive Guide to Benefits Change Form
What is the 2016 Benefits Change Form?
The 2016 Benefits Change Form is essential for associates of Southeast Associates - BCBSNC who wish to modify their health and life insurance benefits. This document enables associates to update their personal information and select medical, dental, vision, and life insurance options. Accurately completing this form is crucial for effective benefits enrollment and to ensure continuous coverage.
Associates must pay close attention when filling out the form, as incorrect submissions may delay or jeopardize their benefits. Understanding the significance of this form is vital for successful benefits management.
Purpose and Benefits of the 2016 Benefits Change Form
The primary purpose of the 2016 Benefits Change Form is to allow associates to modify their employee benefits seamlessly. Associates can adjust their coverage types, such as medical, dental, and vision, ensuring they have the necessary protection for their health and financial security.
Using this form effectively helps in preventing lapses in coverage due to outdated information. Timely updates can alleviate potential disruptions in accessing essential health services.
Who Needs the 2016 Benefits Change Form?
This form is necessary for all associates experiencing significant life changes, such as marriage, divorce, or the birth of a child, who may require adjustments in their coverage options. Additionally, any associate looking to transition to new health plan offerings or alter existing benefits should complete the 2016 Benefits Change Form.
Understanding the specific situations that necessitate this update is crucial for all associates to maintain suitable insurance coverage.
How to Fill Out the 2016 Benefits Change Form Online (Step-by-Step)
Completing the 2016 Benefits Change Form online is straightforward with the following steps:
-
Access the form on the pdfFiller platform.
-
Fill in your personal details, including the Associate Name and Associate ID.
-
Review available coverage options for medical, dental, and vision care.
-
Designate life insurance beneficiaries as required.
-
Apply your digital signature to finalize the form.
Consider your individual needs when selecting coverage options to ensure you make the most informed choices possible.
Field-by-Field Instructions for the Benefits Change Form
To successfully complete the 2016 Benefits Change Form, pay attention to each fillable field:
-
Associate Name: Ensure your full name is entered correctly.
-
Associate ID: Use the identification number provided by your employer.
-
Signature: This is essential for form validation and must be included.
Avoid common mistakes, such as incomplete fields or inaccuracies in personal information, to ensure a smooth submission process.
Digital Signature Requirements for the 2016 Benefits Change Form
When submitting the 2016 Benefits Change Form, both wet signatures and digital signatures are acceptable. Here’s how to apply a digital signature using pdfFiller:
-
Open the form in pdfFiller.
-
Select the signature option to add your digital signature.
-
Save the changes and ensure your signature appears correctly before submission.
Understanding these requirements ensures compliance with verification processes, aiding in the secure handling of your benefits documentation.
Submission Methods for the 2016 Benefits Change Form
Completed forms can be submitted through various methods for convenience and security:
-
Online via pdfFiller for direct submission.
-
Mail to the specified department as outlined in the instructions.
-
In-person at your employer’s human resources office.
To protect your sensitive information, utilize secure submission methods and always double-check that your form is complete.
What Happens After You Submit the Benefits Change Form?
Once submitted, the Benefits Change Form undergoes processing. Generally, it takes a few days to confirm receipt and begin processing the changes. You can track the status of your submission through the designated communication channels.
If any corrections are needed after submission, contact the benefits department immediately to ensure all issues are resolved efficiently.
The Role of pdfFiller in Completing Your 2016 Benefits Change Form
pdfFiller is a powerful tool designed to streamline your experience with the 2016 Benefits Change Form. Its features allow users to edit, fill, and eSign documents with ease, making form management more efficient.
With enhanced security protocols, such as 256-bit encryption, pdfFiller ensures that your personal data remains protected during the form completion process.
Get Started Today with Your 2016 Benefits Change Form
Take the first step towards updating your benefits by utilizing pdfFiller. This service simplifies the process of filling out the 2016 Benefits Change Form, helping you stay on top of your health benefits and ensuring that your coverage remains current.
Embrace the convenience of modern technology to maintain your benefits efficiently.
How to fill out the Benefits Change Form
-
1.Access the 2016 Benefits Change Form on pdfFiller by searching for the document title in the pdfFiller search bar.
-
2.Once opened, familiarize yourself with the form layout, noting all fillable fields, checkboxes, and signature lines.
-
3.Before you begin filling out the form, gather necessary personal information including your Associate Name, Associate ID, and any beneficiary details.
-
4.Start by entering your personal information in the designated fields, ensuring accuracy to avoid processing delays.
-
5.Proceed to select your medical, dental, and vision coverage options by checking the corresponding boxes.
-
6.Designate beneficiaries for your life insurance by filling in their information where prompted.
-
7.After completing all required fields, carefully review the form for any missing information or errors.
-
8.Finalize your form by signing it in the designated signature line, acknowledging your awareness of benefit obligations.
-
9.Once reviewed, save your completed form on pdfFiller to keep a personal copy.
-
10.You can download the form to your device or submit it directly to Delhaize America through the options available on pdfFiller.

Who is eligible to use the 2016 Benefits Change Form?
The 2016 Benefits Change Form is designed for associates of Southeast Associates - BCBSNC who are looking to modify their health and life insurance benefits.
Are there deadlines for submitting the Benefits Change Form?
While specific deadlines are not mentioned, it is advisable to submit the form as soon as possible to ensure timely processing of your benefits changes.
How should I submit the completed form?
After completing the form, you should submit it according to your employer's protocol, typically by returning it directly to Delhaize America via mail or online submission through pdfFiller.
What supporting documents do I need to provide?
You may need to include personal identification details and beneficiary information, but no additional supporting documents are required for the Benefits Change Form itself.
What common mistakes should I avoid when filling out the form?
Common mistakes include leaving fields blank, providing incorrect personal information, or failing to sign the form before submission, all of which could cause delays.
How long does it take to process the Benefits Change Form?
Processing times can vary, but typically expect a few business days after submission for the benefits changes to take effect.
What should I do if I encounter issues with pdfFiller?
If you experience any technical difficulties, refer to the pdfFiller support resources for help or contact their customer support for assistance.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.