Last updated on Apr 4, 2016
Get the free EDI Enrollment Request for Existing Submitter ID
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is EDI Enrollment Form
The EDI Enrollment Request for Existing Submitter ID is a healthcare form used by providers to register for electronic claim submissions with Blue Cross Blue Shield of Alabama.
pdfFiller scores top ratings on review platforms
Who needs EDI Enrollment Form?
Explore how professionals across industries use pdfFiller.

EDI Enrollment Form is needed by:
-
Healthcare providers seeking electronic claims submissions
-
Authorized representatives managing EDI enrollments
-
Billing and coding professionals in healthcare facilities
-
Administrative staff in hospitals and clinics
-
Providers with existing Submitter IDs needing updates
Comprehensive Guide to EDI Enrollment Form
What is the EDI Enrollment Request for Existing Submitter ID?
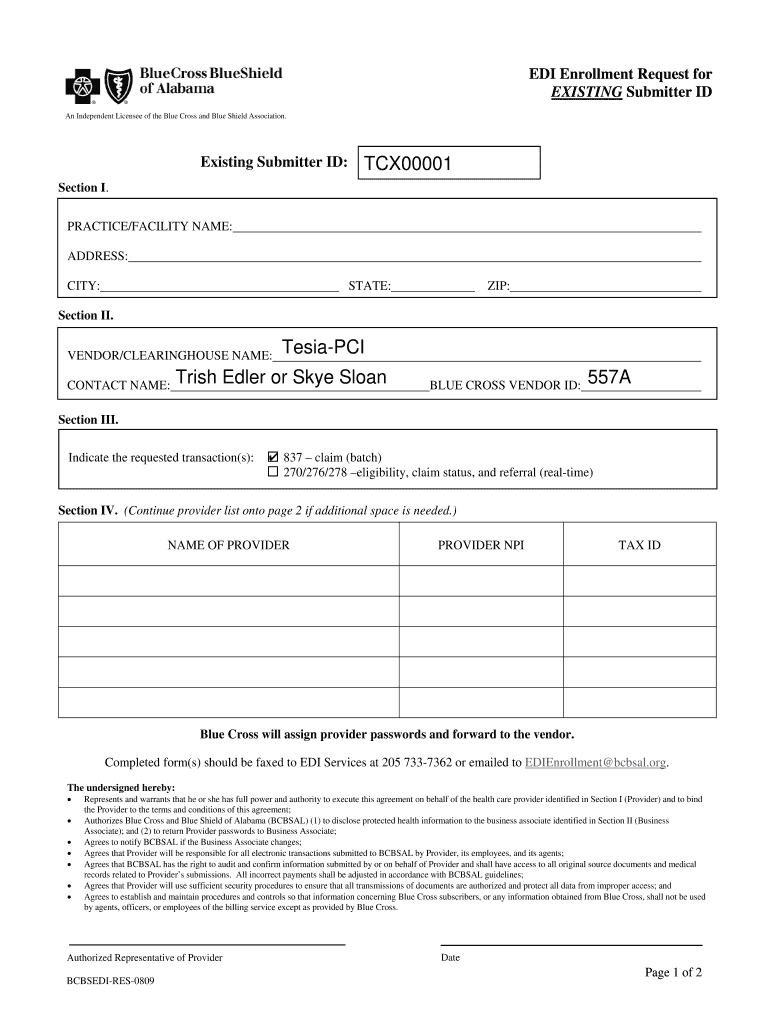
The EDI Enrollment Request for Existing Submitter ID is a crucial form utilized by healthcare providers to register for electronic claim submission with Blue Cross Blue Shield of Alabama. This document serves to streamline the claim submission process, enhancing efficiency and accuracy in transactions.
This form is particularly relevant for healthcare providers operating in Alabama, as it requires specific information including practice or facility details and provider identification. Essential fields include practice or facility name, address, and provider data, which ensure correct processing and communication.
Purpose and Benefits of the EDI Enrollment Request for Existing Submitter ID
Electronic claim submission plays an integral role in the healthcare industry, making it essential for efficient processing and accuracy. By utilizing the EDI Enrollment Request for Existing Submitter ID, providers can facilitate effective communication with Blue Cross Blue Shield of Alabama and ensure quicker claim resolution.
Adding electronic claims into your practice streamlines workflows and reduces the likelihood of errors associated with traditional paper claims. With this form, providers can expedite workflows and improve overall service delivery, ultimately benefiting patients and the healthcare system.
Who Needs the EDI Enrollment Request for Existing Submitter ID?
Authorized representatives of healthcare providers are the primary individuals who must complete the EDI Enrollment Request for Existing Submitter ID. Their signature validates the form and ensures that the submitted information is accurate and legitimate.
This form becomes necessary under specific circumstances for existing submitter IDs, such as when updating information or enrolling in new services under Blue Cross Blue Shield of Alabama.
How to Fill Out the EDI Enrollment Request for Existing Submitter ID Online (Step-by-Step)
-
Access the EDI Enrollment Request form through the designated online platform.
-
Begin by entering your PRACTICE/FACILITY NAME, ensuring all details are correct.
-
Fill in the ADDRESS, CITY, STATE, and ZIP code accurately to avoid processing delays.
-
Provide the NAME OF PROVIDER and any other required identification information.
-
Review your entries for accuracy, then sign the form using blue ink as specified.
Providing precise information is critical, as inaccuracies can lead to rejection or processing delays when submitting the enrollment request.
Submission Methods for the EDI Enrollment Request for Existing Submitter ID
Healthcare providers have multiple channels for submitting the completed EDI Enrollment Request form, including online options and postal services. Depending on your preference, you can choose the most convenient method for your situation.
In Alabama, be mindful of specific delivery options, key deadlines, and processing times to ensure timely submission and acceptance of your request.
Common Errors and How to Avoid Them When Submitting the EDI Enrollment Request
Applicants frequently make various mistakes when filling out the EDI Enrollment Request. Common errors include incorrect provider information and incomplete fields, which can lead to processing delays.
To avoid these issues, ensure you double-check all provided information before submission. Resources may be available for assistance and review, adding an extra layer of security against mistakes.
What Happens After You Submit the EDI Enrollment Request for Existing Submitter ID?
Upon submission of the EDI Enrollment Request, a review process commences to evaluate the accuracy of the provided information. Applicants can expect an acknowledgment of receipt along with instructions on how to track the status of their submission.
Following up on your enrollment status is advisable to ensure confirmation and clarity on next steps in the process.
Security and Compliance in Handling Your EDI Enrollment Request for Existing Submitter ID
Handling sensitive information such as the EDI Enrollment Request for Existing Submitter ID necessitates stringent security measures. Organizations must comply with HIPAA and other relevant privacy regulations to protect patient and provider data.
Implementing best practices for document management, including secure storage and controlled access, will further enhance the privacy and data protection of sensitive submissions.
How pdfFiller Can Help You with the EDI Enrollment Request for Existing Submitter ID
pdfFiller offers substantial advantages for users completing the EDI Enrollment Request for Existing Submitter ID. Its cloud-based platform enables seamless form filling, editing, and eSigning without the need for downloads.
The platform enhances document management, providing features that allow users to keep all necessary documents organized and easily accessible. Utilizing pdfFiller simplifies the process of filling and submitting your healthcare billing forms, ensuring a smooth experience.
Sample Completed EDI Enrollment Request for Existing Submitter ID
A visual example of a filled-out EDI Enrollment Request can provide significant guidance for new applicants. This sample will highlight key sections such as the PRACTICE/FACILITY NAME and NAME OF PROVIDER, making it easier to understand expectations.
Annotations on the sample will point out critical areas to focus on, reinforcing the value of using templates or completed forms to expedite the application process and increase accuracy.
How to fill out the EDI Enrollment Form
-
1.To begin, access pdfFiller and search for the 'EDI Enrollment Request for Existing Submitter ID' form in the template library.
-
2.Once you find the form, click on it to open it in the pdfFiller editor where you can start filling it out.
-
3.Gather required information such as your practice/facility name, address, city, state, ZIP code, and provider name before starting.
-
4.Carefully navigate through the form’s fields, filling in your organization's information and details specific to your vendor or clearinghouse.
-
5.Use the built-in instructions on pdfFiller to ensure proper completion of all fields, including checkboxes for compliance.
-
6.After filling out the form, review all entered information for accuracy, confirming that everything is complete and correctly filled.
-
7.Finalize the form by signing it electronically using blue ink, as mandated for submissions.
-
8.Save your completed form using pdfFiller’s options and choose to download it locally or submit it directly through the platform.

Who qualifies as an authorized representative for signing this form?
An authorized representative must be a designated individual within the healthcare provider organization who has the authority to sign documents related to EDI enrollments. Typically, this could include practice managers or other administrative personnel.
What is the typical processing time for this enrollment request?
Processing times can vary, but generally, you can expect a response within two to four weeks after submission. Ensure that all required fields are correctly filled to avoid delays.
Are there any fees associated with submitting the EDI Enrollment Request?
There are typically no fees for submitting an EDI Enrollment Request with Blue Cross Blue Shield of Alabama; however, checking with the payer for specific cost details is always recommended.
What documents are needed to complete the EDI Enrollment Request?
Generally, you need to provide your existing Submitter ID, facility details, and any vendor or clearinghouse agreements if applicable. It is helpful to have your practice's bank information ready as well.
Can I fill out the form if I do not have a Submitter ID?
No, this form specifically pertains to those with existing Submitter IDs. If you do not have one, you should first complete the initial enrollment process with Blue Cross Blue Shield of Alabama.
What common mistakes should I avoid when completing this form?
Ensure all fields are filled out correctly and do not leave any required sections blank. Avoid using black ink for your signature, as blue ink is specified, which can be a common oversight.
How do I submit the completed EDI Enrollment Request form?
You can submit the form electronically via pdfFiller if the platform supports it, or print the completed document and send it via mail to the designated Blue Cross Blue Shield of Alabama address provided in the form instructions.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.