Last updated on Apr 6, 2016
Get the free HMSA Provider Application Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
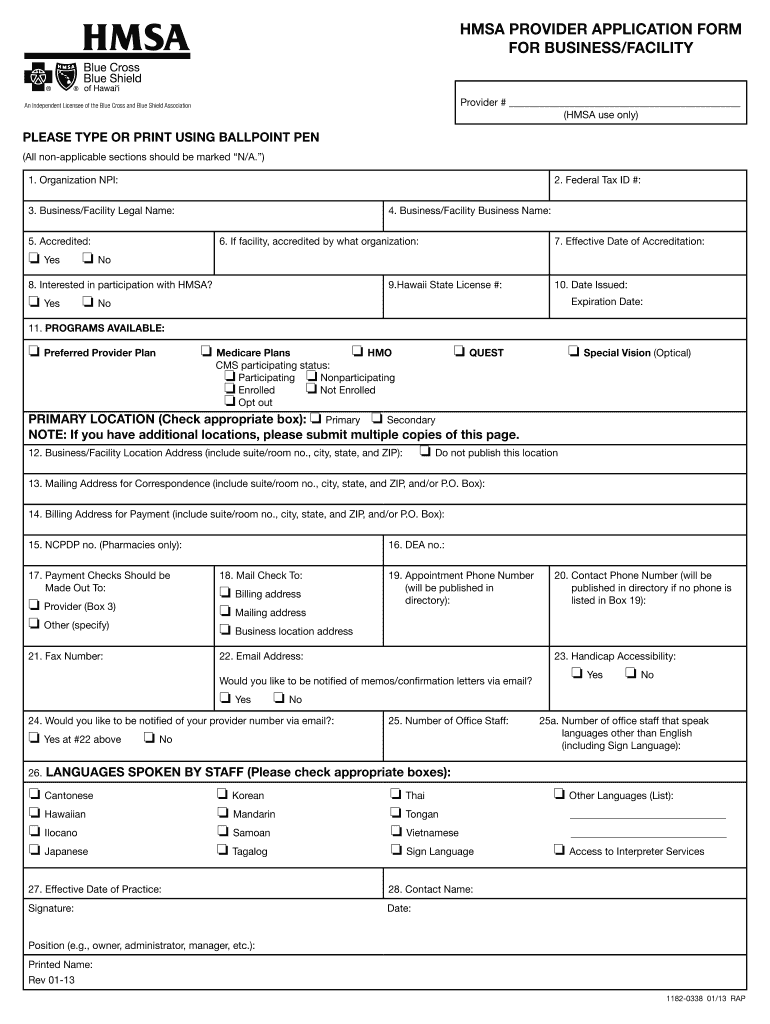
What is HMSA Provider Form
The HMSA Provider Application Form is a healthcare document used by healthcare providers in Hawaii to apply for participation with HMSA (Hawaii Medical Service Association).
pdfFiller scores top ratings on review platforms
Who needs HMSA Provider Form?
Explore how professionals across industries use pdfFiller.

HMSA Provider Form is needed by:
-
Healthcare providers in Hawaii
-
Medical facilities seeking HMSA enrollment
-
Practitioners applying for HMSA participation
-
Administrators handling provider applications
-
Compliance officers for healthcare facilities
Comprehensive Guide to HMSA Provider Form
What is the HMSA Provider Application Form?
The HMSA Provider Application Form is a crucial document for healthcare providers in Hawaii, supporting their application for participation with the Hawaii Medical Service Association (HMSA). This form is designed for various healthcare professionals and facilities eager to join the HMSA network, which plays a vital role in enhancing patient care in the state. By accurately completing this form, providers can begin the process of joining a comprehensive healthcare system that emphasizes quality service delivery.
Purpose and Benefits of the HMSA Provider Application Form
This application process is essential for healthcare providers seeking to participate with HMSA, as it assists in expanding patient access and improving service visibility. The HMSA enrollment form streamlines provider enrollment, allowing for smoother integration into the HMSA system. Additionally, the use of pdfFiller simplifies the application process by providing a user-friendly platform to fill out necessary forms seamlessly.
Who Needs the HMSA Provider Application Form?
The HMSA Provider Application Form is intended for both individual healthcare providers and healthcare facilities. Eligible applicants include physicians, therapists, hospitals, and clinics that wish to extend their services through HMSA. It is important for applicants to understand their eligibility to prevent delays in the application process, ensuring that all necessary roles are considered during submission.
Key Features of the HMSA Provider Application Form
The HMSA Provider Application Form includes several key components that applicants must complete. These components entail:
-
Required fields for organizational details, including legal and business names.
-
Sections for entering tax IDs, accreditation status, and program availability.
-
Contact information, languages spoken, and accessibility considerations.
-
Signatures from authorized representatives
This structured approach ensures that all relevant information is captured efficiently and effectively.
How to Fill Out the HMSA Provider Application Form Online (Step-by-Step)
To complete the HMSA Provider Application Form using pdfFiller, follow these steps:
-
Access the form on pdfFiller's platform.
-
Fill in the required fields, ensuring all information is accurate.
-
Utilize available functionalities to add any additional information or signatures.
-
Review the completed form for accuracy.
-
Submit the application through the platform.
This organized method promotes an efficient filling and signing process, saving time for healthcare providers.
Common Errors and How to Avoid Them
When filling out the HMSA Provider Application Form, there are several frequent mistakes to watch out for, such as:
-
Inaccurate or incomplete contact information.
-
Failure to sign the application.
-
Missing required fields that result in delays.
-
Submitting without reviewing for completeness.
To ensure accuracy, it is crucial to thoroughly review the form before final submission, which helps in speeding up the processing time.
Submission Methods and Delivery for the HMSA Provider Application Form
Healthcare providers can submit the HMSA Provider Application Form in multiple ways, including:
-
Online submission through pdfFiller.
-
Printing the form and delivering it by mail.
Providers must be aware of any specific delivery requirements that apply in Hawaii to ensure successful application processing.
Confirmation and Tracking Your Application Status
Once the completed HMSA Provider Application Form is submitted, providers can confirm receipt through the following steps:
-
Check for an email confirmation, if submitted online.
-
Contact HMSA to inquire about the application status.
-
Keep documentation of submitted forms for personal records.
Monitoring the application's progress is crucial to facilitate necessary follow-up procedures.
Security and Compliance for the HMSA Provider Application Form
In handling the HMSA Provider Application Form, pdfFiller prioritizes security and compliance with significant measures that include 256-bit encryption. This ensures that all sensitive healthcare information remains protected, adhering to HIPAA and GDPR regulations. Healthcare providers can feel confident when using the platform to manage their applications.
Leverage pdfFiller for Your HMSA Provider Application Form Process
Utilizing pdfFiller for managing the HMSA Provider Application Form process offers considerable benefits. The platform enhances the user experience by facilitating efficient document handling, eSigning, and management features. By leveraging these capabilities, healthcare providers can streamline the application process and focus more on delivering quality care.
How to fill out the HMSA Provider Form
-
1.Access pdfFiller and search for the HMSA Provider Application Form to begin. Open the form which will load in the editor.
-
2.Familiarize yourself with the layout of the form and identify the sections that require your information. Use the left navigation panel to jump between sections.
-
3.Gather necessary information such as your organization's legal name, business name, tax ID, and details regarding your accreditation status.
-
4.Start filling in the form fields with the collected information. Click on each fillable field to enter data. Ensure accuracy in all entries to avoid delays.
-
5.Review the contact information section to input your details accurately, including phone numbers and email addresses for correspondence.
-
6.Locate the section for languages spoken and accessibility details. Provide all relevant information to ensure compliance with HMSA requirements.
-
7.Once all sections are completed, review the entire form carefully for any missing information or errors. Use the preview option to view your form as it will appear when finalized.
-
8.After confirming all information is correct, scroll to the bottom of the form to sign electronically using pdfFiller's signature tool.
-
9.Finally, choose to save, download, or submit the completed form directly through pdfFiller, following any additional prompts for submission. You may also receive an email confirmation after submission.

Who is eligible to apply using the HMSA Provider Application Form?
Healthcare providers and medical facilities in Hawaii seeking participation with HMSA are eligible to use the HMSA Provider Application Form. Ensure your organization meets HMSA's participation criteria before applying.
What information is required before completing the application?
Before starting the application, gather your organization's legal name, business name, tax ID number, accreditation status, and details on available programs you offer. This information is crucial for a complete application.
Are there any submission deadlines for the form?
While specific deadlines aren't mentioned, it's advisable to submit the HMSA Provider Application Form as soon as possible to avoid delays in enrollment. Check HMSA's official guidelines for potential cut-off dates.
How do I submit the HMSA Provider Application Form?
You can submit the HMSA Provider Application Form electronically via pdfFiller. Follow the prompts to complete signing, and choose to submit directly from the platform after filling in all necessary information.
What common mistakes should I avoid when completing the form?
Ensure all fields are filled out completely and accurately. Avoid leaving required fields blank and double-check your contact information. Missing details may result in processing delays.
What is the processing time for the HMSA Provider Application Form?
Processing times for the HMSA Provider Application Form can vary. Typically, you should expect a few weeks for review and approval. Check directly with HMSA for the most accurate timelines.
Do I need to notarize the HMSA Provider Application Form?
No, you do not need to notarize the HMSA Provider Application Form. However, it must be signed by an authorized representative of your organization.
Related Forms


Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.