Last updated on Apr 9, 2016

Get the free Patient Information Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
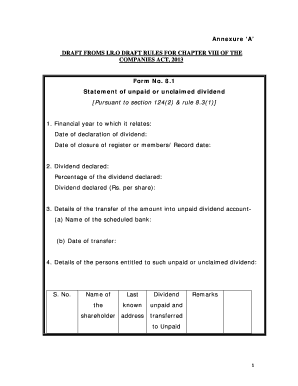
What is Patient Info Form
The Patient Information Form is a medical history document used by healthcare providers to collect essential patient details for registration and treatment consent.
pdfFiller scores top ratings on review platforms
Who needs Patient Info Form?
Explore how professionals across industries use pdfFiller.

Patient Info Form is needed by:
-
New patients registering at healthcare facilities
-
Healthcare providers needing accurate patient records
-
Insurance companies requiring patient information
-
Administrators managing patient intake
-
Emergency contacts listed by patients
-
Clinics ensuring compliance with patient consent laws
Comprehensive Guide to Patient Info Form
Understanding the Patient Information Form
The Patient Information Form is a critical document in healthcare, serving as a comprehensive record that gathers essential details about new patients. By compiling personal information, medical history, and insurance details, healthcare providers can ensure the accuracy of patient records and facilitate efficient billing processes. Accurate data collection helps avoid complications and delays in treatment.
Utilizing this medical history form allows healthcare professionals to create informed care plans tailored to each patient's unique needs, demonstrating the importance of the Patient Information Form in streamlined healthcare delivery.
Purpose and Benefits of the Patient Information Form
This form is essential for a variety of reasons, primarily focusing on improving the healthcare registration process for both patients and providers. Healthcare providers request this form to gather vital information that can influence treatment decisions and billing complexities.
-
Streamlined registration for new patients, making the check-in process more efficient.
-
Informed care provision based on accurate medical histories provided by patients.
By filling out the patient consent form, individuals take the first step in their healthcare journey, allowing for enhanced communication and better service delivery.
Who Needs the Patient Information Form?
The primary users of the Patient Information Form include new patients seeking care and healthcare providers requiring up-to-date records. This form is particularly necessary during initial visits when a healthcare provider begins the patient intake process.
Additionally, scenarios such as changes in health status or insurance details warrant the completion of this form to ensure that any updates are captured accurately, facilitating seamless healthcare delivery.
How to Fill Out the Patient Information Form Online
Completing the Patient Information Form online is straightforward if you follow these steps:
-
Gather personal information including full name, date of birth, and contact details.
-
Prepare your medical history, including past illnesses, surgeries, and any ongoing treatments.
-
Have your insurance information ready to provide complete details regarding coverage.
Each section of the form will prompt you for specific information, ensuring that nothing crucial is overlooked. By following these steps, you will contribute to a smooth healthcare registration process.
Common Errors and Tips for Avoiding Mistakes
When completing the Patient Information Form, users may encounter several common mistakes. Recognizing these can help ensure accurate submission:
-
Forgetting to fill out mandatory fields, which can delay the registration process.
-
Providing incorrect insurance information, potentially affecting coverage.
-
Omitting important medical history details that can impact treatment.
To avoid these errors, take your time to review the form thoroughly before submission, ensuring all information is complete and accurate.
Review and Validation Checklist for the Patient Information Form
Prior to submitting the Patient Information Form, users should perform a thorough review. Key points to check include:
-
All personal and medical information is correctly entered and up-to-date.
-
Insurance details match those provided by your provider to avoid conflicts.
-
Your signature is included, authorizing treatment and billing.
This validation step is critical for ensuring the integrity of your healthcare information, ultimately enabling timely and effective care.
How to Sign the Patient Information Form
Signing the Patient Information Form is an important step that confirms your consent to the terms outlined in the document. Understanding the differences between digital and wet signatures can be beneficial:
-
Digital signatures provide a secure method of signing online, often required for electronic submissions.
-
Wet signatures are traditional and may be necessary in certain circumstances where digital forms are not accepted.
Both types of signatures serve to authenticate your approval for treatment, ensuring your healthcare provider can proceed with the necessary care.
Digital Solutions for Completing Your Patient Information Form
pdfFiller offers a convenient solution for completing the Patient Information Form, allowing users to fill out and sign the document securely online. With features tailored for this form, users can expect:
-
A user-friendly interface for easy form completion.
-
Strong security measures, including HIPAA and GDPR compliance, to protect sensitive information.
This platform is designed to streamline the process while ensuring that all personal data remains confidential and secure.
What Happens After You Submit the Patient Information Form?
Once you submit the Patient Information Form, processing typically begins immediately. Here’s what to expect:
-
Healthcare providers will review the information to ensure it is complete and accurate.
-
You may receive a follow-up call or email for any necessary clarifications or additional information.
If corrections or amendments to the form are needed, providers will guide you through the process, ensuring that all records remain up-to-date.
Explore More Healthcare Forms with pdfFiller
pdfFiller also provides a platform to easily create, edit, and manage various healthcare-related documents. Leveraging this tool can help streamline additional healthcare registration processes.
Users can benefit from a secure environment to handle multiple forms and enhance overall efficiency in managing their healthcare documentation.
How to fill out the Patient Info Form
-
1.To begin, access pdfFiller and locate the Patient Information Form in the form library.
-
2.Open the form by selecting it from your saved documents or searching using the form title.
-
3.Before you start filling out the form, gather your personal information like full name, address, phone number, and email address.
-
4.Navigate through the form's fields using your mouse or keyboard, clicking on each field to input your information.
-
5.Fill in your medical history by answering the relevant questions, providing information regarding past illnesses, surgeries, and medications.
-
6.Complete the sections for insurance information by entering your insurer’s name, policy number, and any other required details.
-
7.If there are fields that require checkboxes, ensure you click to select the appropriate options.
-
8.Once all sections are completed, review your entries for accuracy, making corrections where needed.
-
9.Check that you have signed the form where indicated, ensuring you authorize payment and consent to treatment.
-
10.Finally, save your completed form to your pdfFiller account, download it for local storage, or submit it directly to your healthcare provider through the submission options available.

Who is eligible to fill out the Patient Information Form?
The Patient Information Form is intended for new patients registering with healthcare providers who require accurate information to create patient records and consent to treatment.
What information do I need to complete the form?
You will need personal details such as your name, address, phone number, insurance information, and your medical history including past illnesses and medications.
How do I submit the Patient Information Form?
The form can be submitted electronically through pdfFiller, downloaded for print and physical submission, or directly sent to your healthcare provider via email.
Are there any common mistakes to avoid when completing the form?
Common mistakes include omitting essential information, not signing the form, and failing to double-check insurance details. Review each section carefully before submission.
How long does it take to process the Patient Information Form?
Processing time for the form is typically quick, often completed within a few days, depending on the healthcare provider's intake process and workload.
What happens if I don’t have insurance information?
If you do not have insurance information, leave that field blank or indicate 'self-pay' if applicable. Discuss alternatives with your healthcare provider.
Can I edit the form after it has been submitted?
Once submitted, you may need to contact your healthcare provider to make any edits or corrections. It's best to ensure all information is accurate before submission.
Related Forms


Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.