Last updated on Apr 13, 2016
Get the free Authorization to Release Patient Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Patient Info Release
The Authorization to Release Patient Information is a medical records release form used by patients or their legal representatives to consent to the disclosure of medical records.
pdfFiller scores top ratings on review platforms
Who needs Patient Info Release?
Explore how professionals across industries use pdfFiller.

Patient Info Release is needed by:
-
Patients needing access to their medical records.
-
Parents or legal guardians of minors requiring medical data.
-
Legal representatives managing patient information temporarily.
-
Witnesses assisting in verifying the authenticity of the signatures.
-
Healthcare professionals requesting patient data for treatment.
Comprehensive Guide to Patient Info Release
What is the Authorization to Release Patient Information?
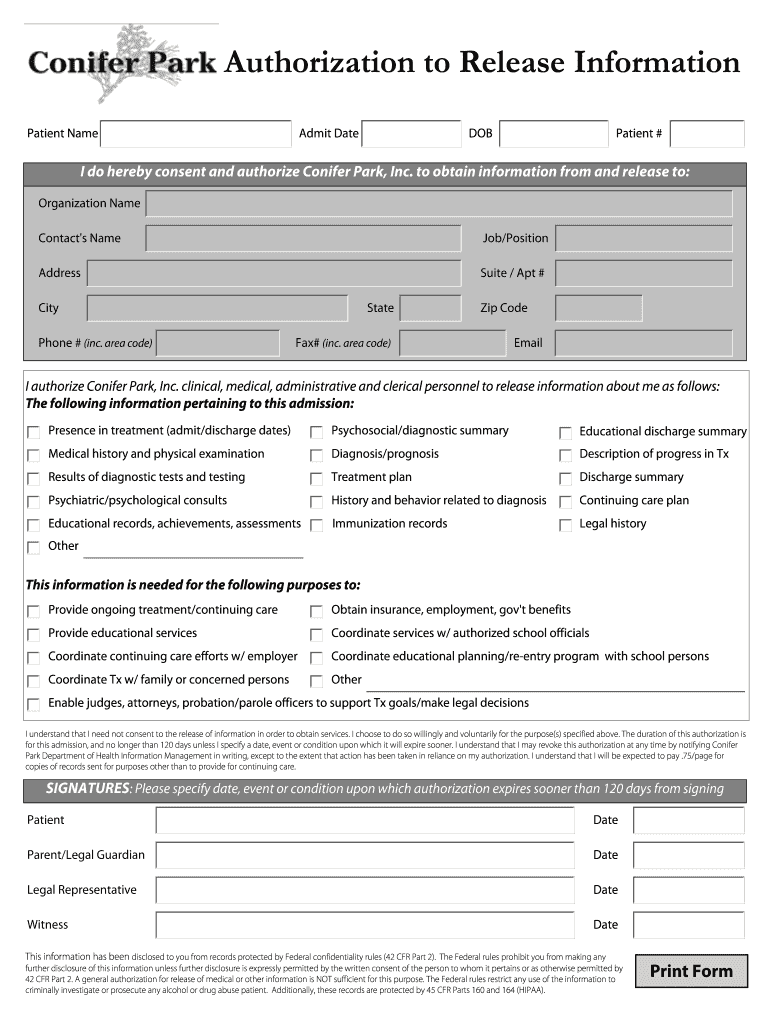
The Authorization to Release Patient Information is a crucial document in the healthcare sector. This form allows patients, or their legal representatives, to grant permission for the release of medical records. Specifically, Conifer Park, Inc. facilitates this process by ensuring compliance with healthcare regulations and safeguarding patient rights. Understanding this form is essential, as it ensures that sensitive patient information is disclosed appropriately and legally.
Purpose and Benefits of the Authorization to Release Patient Information
This authorization form is vital for protecting patient rights and ensuring that information is shared responsibly. A signed document secures patient consent and facilitates the lawful disclosure of health information. The benefits include improved communication among healthcare providers, expedited access to essential medical records for treatment purposes, and enhanced clarity for families during medical decision-making. By using a standardized healthcare authorization form, everyone involved can enjoy a straightforward approach to patient information disclosure.
Who Needs the Authorization to Release Patient Information?
The signing of the Authorization to Release Patient Information involves several key roles, each carrying specific responsibilities. These roles include:
-
Patient: The primary individual whose medical records are being released.
-
Parent/Legal Guardian: Responsible for providing consent on behalf of minors.
-
Legal Representative: Authorized to act on behalf of patients for various legal matters.
-
Witness: Validates the authenticity of the signatures on the form.
Each role plays a vital part in ensuring compliance with regulations like HIPAA, which governs medical records consent.
Key Features of the Authorization to Release Patient Information
The Authorization to Release Patient Information form is designed with several key components that facilitate its use. Fillable sections include:
-
Patient Name
-
Admit Date
-
Date of Birth (DOB)
-
Patient Number
Additionally, the form includes signature lines for all required roles and checkboxes for specifying the types of information being released. This clear structure reduces confusion when completing the form.
How to Fill Out the Authorization to Release Patient Information Online
Filling out the Authorization to Release Patient Information online is a straightforward process. Follow these steps to ensure correct completion:
-
Access the online form and input the patient’s demographic information in the designated fields.
-
Review the list of parties to whom the information will be released and check the appropriate boxes.
-
Provide the required signatures, ensuring they are legible.
-
Double-check all entries for accuracy.
Common errors to avoid include missing required fields and inconsistent signing. Each step is crucial to ensure the form is valid and effective.
Submission Methods and Delivery for the Authorization to Release Patient Information
Once the form is completed, there are several methods for submission. These include:
-
Online submission via a secure portal
-
Mailing the completed form to the designated address
-
Delivering the form in person to the appropriate healthcare provider
After submission, confirmation and tracking options may be available to ensure the form has been received and processed in a timely manner.
Security and Compliance When Using the Authorization to Release Patient Information
Data protection is essential when handling the Authorization to Release Patient Information. Security measures include:
-
256-bit encryption for data transmission
-
Compliance with HIPAA regulations to protect patient privacy
To maintain confidentiality, it's crucial to handle this sensitive document with care, ensuring it's only accessed and shared by authorized individuals.
Example of a Completed Authorization to Release Patient Information
Providing a sample or example of a completed Authorization to Release Patient Information form can greatly assist users. An example illustrates how to accurately fill in key sections and common data entries, highlighting areas such as:
-
Correctly entering the patient’s full name
-
Ensuring all required signatures are obtained
This visual reference helps to alleviate confusion and ensures compliance with the form's requirements.
Enhance Your Experience with pdfFiller
pdfFiller offers a user-friendly platform for completing the Authorization to Release Patient Information. Key features include:
-
Editing tools to adjust text and images
-
eSigning capabilities for quick and secure signatures
This solution guarantees ease of use while ensuring secure document management, making it an ideal choice for patients and providers alike.
How to fill out the Patient Info Release
-
1.To access the Authorization to Release Patient Information form on pdfFiller, go to the pdfFiller website and search for the form using its name or relevant keywords.
-
2.Once you have found the form, click on it to open the interactive editing interface provided by pdfFiller.
-
3.Begin by filling in the 'Patient Name', 'Admit Date', 'DOB', and 'Patient #' fields. Ensure all information is accurate and up-to-date.
-
4.As you complete the form, use the provided boxes to check off what information will be released and to whom it will be disclosed.
-
5.Gather any necessary documents that verify your identity and authorization, such as legal guardianship papers or power of attorney documents, before completing the form.
-
6.Once you finish filling out the required fields, review all information carefully to avoid common mistakes, ensuring signatures are obtained where necessary.
-
7.To finalize the form, follow the prompts to save it. You can choose to download it, print it, or submit it through pdfFiller’s platform as needed.

Who is eligible to fill out the Authorization to Release Patient Information?
Eligibility includes patients themselves, parents or legal guardians of minor patients, and legal representatives holding proper authority to sign on behalf of the patient.
How long is the authorization valid?
The authorization is valid for up to 120 days, unless specified otherwise in the document. Ensure to indicate the duration if it differs from the standard.
How do I submit the form after filling it out?
You can save and download the completed form through pdfFiller. Alternatively, it can be directly submitted to the healthcare provider as specified in the instructions.
Are there any supporting documents needed when submitting the form?
Yes, it’s advisable to attach any necessary identification documents or legal papers that support your role as a signer, such as guardianship documents or legal authority letters.
What are common mistakes to avoid when filling out this form?
Common mistakes include missing signatures, incorrect patient information, and not specifying the limits of information being released. Double-check all entries before submission.
How can I move through the form fields on pdfFiller?
Use your mouse or tab key to navigate between fields on pdfFiller. Interactive prompts will guide you to the next editable sections.
What should I do if I need to make changes after submitting?
If you need to make changes after submission, contact the receiving party directly to discuss the necessary modifications. Most processes allow for amendments if justified.
Related Forms









Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.