Last updated on Apr 13, 2016

Get the free Authorization to Use/Disclose Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
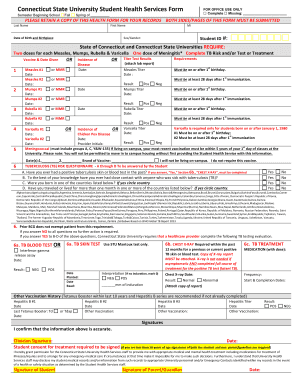
What is Health Info Authorization
The Authorization to Use/Disclose Health Information is a healthcare form used by patients in Oregon to grant permission for the use and disclosure of their health information.
pdfFiller scores top ratings on review platforms
Who needs Health Info Authorization?
Explore how professionals across industries use pdfFiller.

Health Info Authorization is needed by:
-
Patients seeking to authorize the release of their health information
-
Medical professionals requiring access to patient records
-
Legal representatives managing patient health information
-
Healthcare facilities involved in treatment and care
-
Insurance companies needing health information for claims processing
Comprehensive Guide to Health Info Authorization
What is the Authorization to Use/Disclose Health Information?
The Authorization to Use/Disclose Health Information form is a crucial document that enables individuals to grant permission for the management and dissemination of their health information. This form allows patients to control access to their sensitive medical data, ensuring that only authorized parties can use or disclose it. Granting consent is essential for maintaining privacy in healthcare, and this authorization specifically identifies the types of health information that may be shared, such as medical history and test results. By completing this form, patients protect their right to confidentiality while supporting necessary healthcare communications.
Purpose and Benefits of the Authorization to Use/Disclose Health Information
Patients need to authorize disclosures of their health information for various reasons, primarily to facilitate effective healthcare and ensure that providers have the necessary data for proper treatment. This form provides several benefits, including:
-
Streamlining communication between patients and healthcare providers.
-
Reassuring patients that their sensitive information is handled properly.
-
Making it easier for patients to manage their medical records and healthcare decisions.
By utilizing the Authorization to Use/Disclose Health Information, both patients and providers can experience a more organized approach to managing patient health records consent.
Key Features of the Authorization to Use/Disclose Health Information
The Authorization to Use/Disclose Health Information is designed with several essential features that cater to user needs:
-
Fillable fields for the patient's name, date of birth, and signature.
-
An option to specify sensitive health information, such as conditions related to HIV or mental health.
-
A defined duration of validity, typically 180 days, with options for further disclosures.
These features ensure that the form meets the diverse requirements of both patients and healthcare providers, paving the way for responsible health information management.
Who Needs the Authorization to Use/Disclose Health Information?
This authorization is essential for various individuals and situations. Typically, authorization is required from patients, healthcare providers, and caregivers. The form plays a critical role when:
-
Patients switch doctors and need to transfer their medical records.
-
Submitting claims to insurance providers for reimbursement.
-
Family members or caregivers manage the healthcare of individuals who cannot make decisions on their own.
The usage of this form is key to ensuring that health information is disclosed appropriately while respecting patient privacy.
How to Fill Out the Authorization to Use/Disclose Health Information Online
Filling out the Authorization to Use/Disclose Health Information online can be straightforward. Follow these step-by-step instructions:
-
Access the form on a reliable platform, such as pdfFiller.
-
Enter personal details, including the patient's name and date of birth.
-
Specify any sensitive health information that needs authorization.
-
Review the form for accuracy and completeness.
-
Sign the form electronically, if required.
Be aware of common pitfalls, such as leaving required fields empty or providing incorrect information. Completing these steps carefully helps ensure the authorization is accepted without delays.
Submission Methods for the Authorization to Use/Disclose Health Information
Once the form is completed, users can submit it through various methods, depending on preferences and provider requirements:
-
Online submission via secure healthcare portals.
-
Mailing the form to the designated healthcare provider's address.
-
Hand-delivering the form in person to the healthcare facility.
It's important to be aware of deadlines and expected processing times, which can vary based on the submission method and recipient.
Security and Compliance for the Authorization to Use/Disclose Health Information
Ensuring data security and compliance with privacy regulations is paramount in the management of health information. The key regulations include:
-
The Health Insurance Portability and Accountability Act (HIPAA).
-
The implementation of robust security measures to protect sensitive documents.
-
The need to safeguard personal health data throughout the disclosure process.
Healthcare providers and patients must remain vigilant about these security protocols to maintain the integrity of personal health information.
What Happens After You Submit the Authorization to Use/Disclose Health Information?
After submitting the Authorization to Use/Disclose Health Information, users should expect a confirmation of receipt. Here are some possible outcomes:
-
Immediate confirmation that the authorization has been accepted.
-
Notification of any issues that could delay the processing of the form.
-
Timeframes for when users can expect a response or further actions required.
If authorization is not accepted, it is crucial to understand the steps needed to rectify any issues that arise.
Utilizing pdfFiller for Your Authorization to Use/Disclose Health Information Needs
pdfFiller is an excellent solution for managing the Authorization to Use/Disclose Health Information. This platform offers a range of benefits:
-
A user-friendly interface for filling, signing, and submitting the form seamlessly.
-
Tools to ensure compliance with relevant regulations and security standards.
-
Features that simplify the entire process of document management, from editing to sharing.
By leveraging pdfFiller, users can handle their health information needs with ease and confidence, ensuring that sensitive data remains secure throughout the process.
How to fill out the Health Info Authorization
-
1.Access the Authorization to Use/Disclose Health Information form by navigating to pdfFiller and searching for the specific document title.
-
2.Once the form is open in pdfFiller, review the introductory sections to understand the information required.
-
3.Before filling in the fields, gather necessary information such as your name, date of birth, and specifics of the health records needed.
-
4.Using pdfFiller's interface, begin filling in your personal details in the designated fields provided.
-
5.Make selections in the checkboxes regarding any sensitive information, like mental health or genetic testing, as needed.
-
6.Double-check that all fields are filled out accurately to avoid processing delays.
-
7.After completing the form, thoroughly review all sections again to ensure everything is entered correctly.
-
8.Once satisfied, use the save option to keep a copy of your completed form on pdfFiller.
-
9.You can then download the finished form or submit it directly to the required entity using pdfFiller's submission features.

Who is eligible to use the Authorization to Use/Disclose Health Information form?
The form is primarily for patients in Oregon who wish to authorize the disclosure of their health information to specific parties.
What should I do if I need to submit the form by a certain date?
Ensure to complete and submit the Authorization form well in advance of any deadlines, allowing time for processing. The form is valid for 180 days once signed.
How do I submit the completed Authorization form?
After filling the form on pdfFiller, you can either download it for physical submission or submit it directly through electronic means if applicable.
What supporting documents are required with this Authorization form?
Typically, you will need to provide proof of identity, such as a government-issued ID, along with the completed Authorization form to facilitate the process.
What are common mistakes to avoid when completing this form?
Ensure you accurately fill out all required fields and double-check for any misspellings or missing information, as these can delay the authorization process.
How long does it take to process the Authorization to Use/Disclose Health Information form?
Processing times can vary based on the entity receiving the request; allow sufficient time for completion and retrieval of your health information.
What if I change my mind after signing the Authorization form?
You can revoke the authorization at any time before it is executed by notifying the entity that received the authorization in writing.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.