Last updated on Apr 13, 2016
Get the free Authorization to Release Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
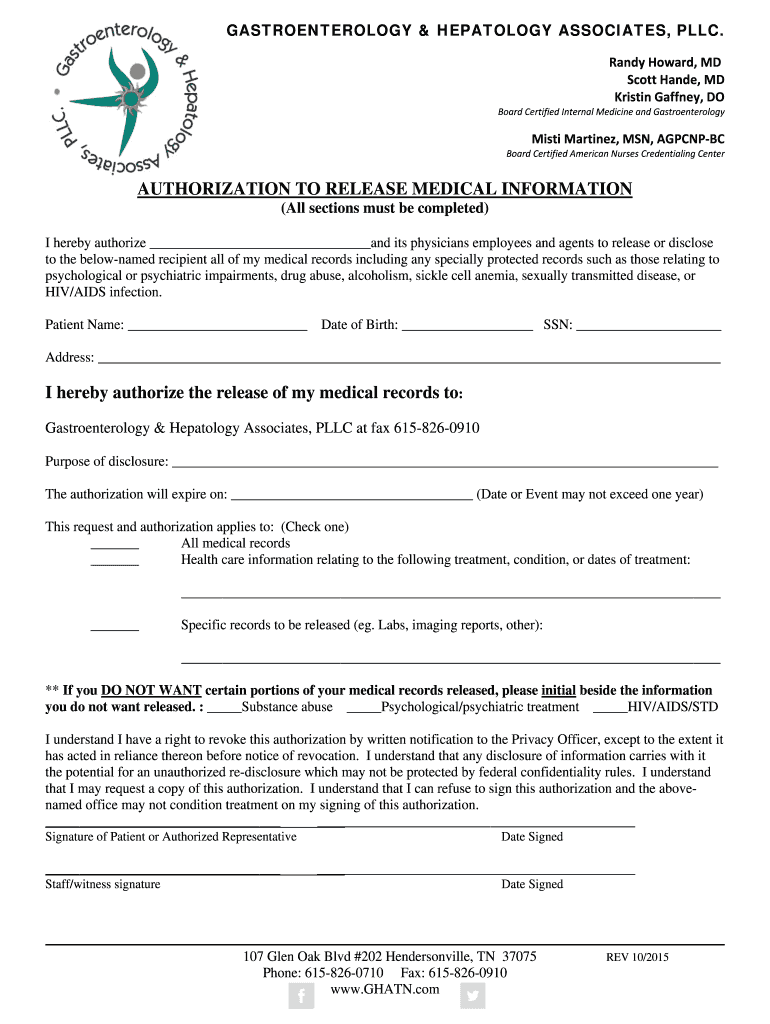
What is Medical Release Form
The Authorization to Release Medical Information is a healthcare form used by patients to grant permission for the release of their medical records to designated recipients.
pdfFiller scores top ratings on review platforms
Who needs Medical Release Form?
Explore how professionals across industries use pdfFiller.

Medical Release Form is needed by:
-
Patients seeking to share their medical records with healthcare providers
-
Medical professionals requiring patient consent for record access
-
Staff members responsible for processing medical releases
-
Legal representatives managing patient health information
-
Healthcare organizations needing authorization for record sharing
Comprehensive Guide to Medical Release Form
What is the Authorization to Release Medical Information?
The Authorization to Release Medical Information is a crucial document in healthcare that allows patients to provide consent for the release of their medical records to specified individuals or entities. This form plays a vital role in safeguarding patient privacy while facilitating necessary medical communications.
Patient consent is essential as it ensures that healthcare providers adhere to legal standards, allowing patients to control who accesses their sensitive health information. Key terms related to this authorization include "medical release form" and "patient consent form," which highlight its purpose in the context of patient rights.
Purpose and Benefits of the Authorization to Release Medical Information
This authorization is necessary to ensure that patient information is shared securely and only with authorized parties. One of the primary benefits of this form is that it fosters effective communication between patients and medical professionals, particularly when patients are seeking treatment from multiple providers or during transitions of care.
There are various scenarios where the release of medical information becomes critical, such as during a referral, insurance claim submission, or coordination with specialists. Using the "HIPAA authorization form" can help protect patient rights while effectively managing medical records release, which is essential for quality patient care.
Key Features of the Authorization to Release Medical Information
The Authorization to Release Medical Information includes several key features designed to enhance usability and compliance. These features comprise distinct sections such as recipient details, types of medical records to be released, and any exclusions pertinent to the patient’s sensitive information.
Each fillable field within the form serves a specific purpose, ensuring accurate information collection. It also mandates signatures from both the patient and a staff member, thereby reinforcing compliance and validation of the authorization process.
Who Needs the Authorization to Release Medical Information?
This form is primarily intended for patients or authorized representatives who wish to control the dissemination of their medical records. The individuals who usually complete the form include patients seeking to share information with new healthcare providers or representatives managing medical affairs on behalf of patients.
Submitting the authorization may be necessary in circumstances such as transferring medical records from one provider to another or when patients wish to provide records to insurance companies. In these situations, utilizing a "patient consent form" can streamline the "medical records release" process efficiently.
How to Fill Out the Authorization to Release Medical Information (Step-by-Step)
Filling out the Authorization to Release Medical Information requires attention to detail to ensure the form is completed accurately. Start by entering your name, date of birth, and Social Security Number (SSN) as required in the designated fields.
After providing personal identifiers, specify the purpose for disclosing your medical records. If there are specific medical records you wish to exclude from the release, outline those clearly as well. Follow these steps to ensure you have accurately filled out the form without omissions:
-
Enter your full name.
-
Provide your date of birth.
-
Fill in your Social Security Number.
-
Specify the purpose of disclosure.
-
Complete the recipient information.
-
Sign and date the form.
Security and Compliance for the Authorization to Release Medical Information
Ensuring security and compliance is paramount when dealing with the Authorization to Release Medical Information. pdfFiller provides comprehensive solutions to safeguard sensitive medical documents by fully complying with HIPAA and GDPR regulations.
The platform employs robust security measures for digital submissions and offers digital signatures, ensuring that patient information is handled with the utmost care. Prioritizing "privacy and data protection" is critical for both patients and healthcare providers using a "medical release form."
Submitting the Authorization to Release Medical Information
Submitting the Authorization to Release Medical Information can be done through several methods, depending on what is most convenient for the patient. Options include online submissions via pdfFiller, as well as in-person or by mail submissions to the designated healthcare provider.
It is important for patients to be aware of any potential fees associated with processing the form, as well as deadlines for submission and expected processing times. Knowing "when to file the form" and understanding the available "submission methods" can greatly assist in expediting the release of medical information.
Common Errors and How to Avoid Them
Completing or submitting the Authorization to Release Medical Information can come with challenges if not approached with diligence. Some frequent errors include missing signatures or providing incomplete fields, which can lead to delays or rejections.
To mitigate these issues, it is advisable to conduct a thorough review of the form before finalization. A checklist can be useful to ensure all necessary information has been completed accurately. Common rejection reasons often stem from the following mistakes:
-
Omitting required signatures.
-
Failing to provide necessary details in fillable fields.
-
Incorrectly specifying the records to be shared.
Sample or Example of a Completed Authorization to Release Medical Information
A visual reference can significantly aid in understanding how to complete the Authorization to Release Medical Information correctly. An annotated example of a fully completed form showcases proper entry of information, ensuring all required details are provided systematically.
This example illustrates the significance of each section, demonstrating how fields should be filled to adhere to compliance standards effectively. Reviewing this example can offer valuable insights into "medical records release" and the importance of correctly managing the "authorization to release medical information."
Empower Your Document Management with pdfFiller
Utilizing pdfFiller for your document management simplifies the process of filling out and submitting the Authorization to Release Medical Information. The platform features tools that enhance usability, making it easier to complete the form accurately and securely.
Emphasizing the benefits of a cloud-based service, pdfFiller ensures sensitive documents are managed with high security. With user-friendly features and robust security protections, pdfFiller stands out in the market as an ideal solution for managing medical records and sensitive information.
How to fill out the Medical Release Form
-
1.To begin, visit pdfFiller and log into your account or create a new one if you don’t have one already. Use the search bar to locate the Authorization to Release Medical Information form quickly.
-
2.Once you have opened the form, familiarize yourself with the fillable fields. Start by entering your personal information, including your name, date of birth, Social Security Number (SSN), and address in the designated areas.
-
3.Ensure that you have all necessary documentation on hand. This should include identification documents and any relevant medical records that will help you specify the details required in the form.
-
4.After filling out the personal information, review the sections where you can indicate the purpose of disclosure and the specific medical records you are authorizing for release. Be detailed and precise to avoid any misunderstanding.
-
5.Next, read through the authorization clauses carefully. Make sure you understand the information being shared and that you are comfortable with who will receive your medical records.
-
6.Sign the form electronically using pdfFiller's signature tool. If you are signing on behalf of a patient, ensure you have the necessary authority to do so, and enter your signature.
-
7.Finally, have the form witnessed by a staff member as required. Once everything is completed, review your entries for accuracy.
-
8.Save the completed form by clicking the save option in pdfFiller. You can also download it as a PDF or submit it directly through the platform if required by your healthcare provider.

Who is eligible to use the Authorization to Release Medical Information form?
Any patient seeking to authorize the release of their medical records to specified recipients is eligible to use this form. An authorized representative can also complete it on the patient's behalf.
Are there deadlines for submitting the Authorization to Release Medical Information?
While there are generally no strict deadlines for submitting this form, it’s advisable to submit it as soon as possible, especially if time-sensitive medical needs arise.
How do I submit the completed Authorization to Release Medical Information form?
You can submit the completed form by downloading it and providing it to your healthcare provider, or you may submit it electronically if your provider accepts digital submissions.
What supporting documents do I need to provide with this form?
Typically, you will need to provide identification, such as a driver's license or passport, to verify your identity and authority to release the medical information.
What common mistakes should I avoid when filling out this form?
Ensure that all personal information is accurate, that you include all necessary signatures, and that you specify the medical records and recipients clearly to avoid delays in processing.
How long does it take to process the Authorization to Release Medical Information form?
Processing times can vary based on the healthcare provider's policies; it may take a few days to up to two weeks. It’s recommended to check directly with the provider for their specific timelines.
Can I revoke my consent after submitting this form?
Yes, you can revoke your consent at any time by notifying the healthcare provider in writing, but keep in mind that any disclosures made prior to the revocation will still be valid.
Related Forms








Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.