Last updated on Apr 14, 2016
Get the free Dental Provider Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Dental Request Form
The Dental Provider Request Form is a healthcare document used by dental providers in Arkansas to request coordinated care services for beneficiaries.
pdfFiller scores top ratings on review platforms
Who needs Dental Request Form?
Explore how professionals across industries use pdfFiller.

Dental Request Form is needed by:
-
Dental providers seeking coordinated care for patients
-
Medicaid beneficiaries requiring dental services
-
Healthcare administrators managing dental appointments
-
Transportation services assisting patients with appointments
-
Beneficiary family members coordinating care details
Comprehensive Guide to Dental Request Form
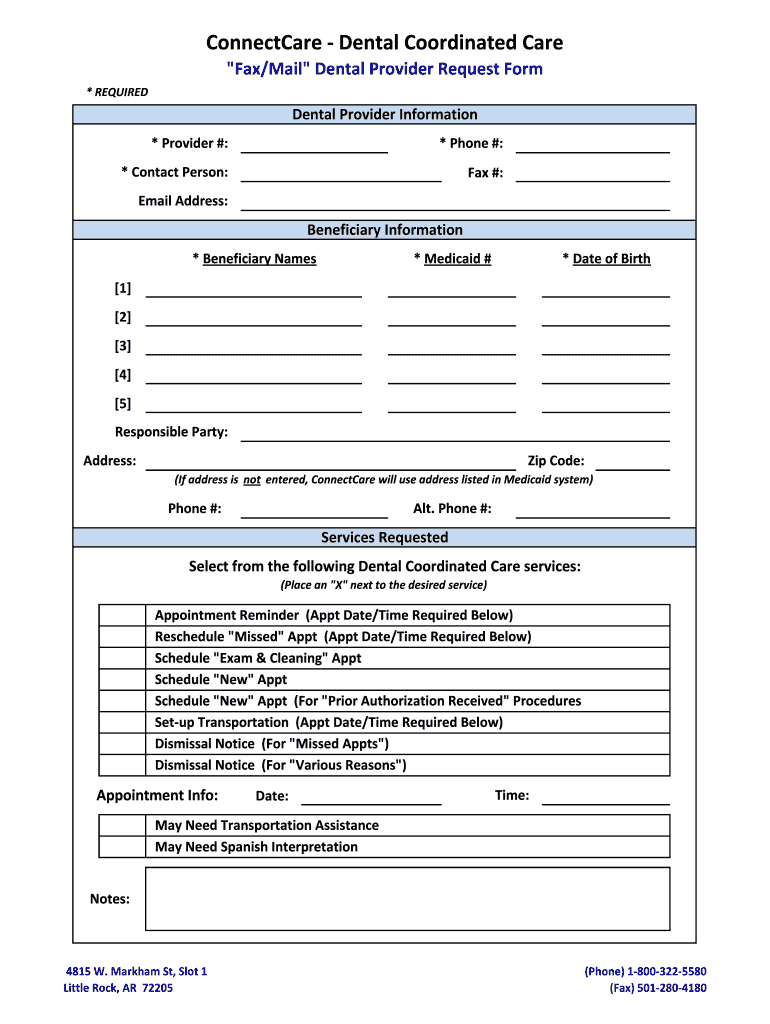
What is the Dental Provider Request Form?
The Dental Provider Request Form is a critical document used by dental providers in Arkansas to request coordinated care services for Medicaid beneficiaries. This form enables providers to submit essential information regarding patient needs and service requests, ensuring that clients receive necessary care.
This form is primarily utilized by dental providers who cater to Medicaid beneficiaries, making it a significant part of the healthcare system in Arkansas. Its role is vital as it facilitates communication and coordination among care providers.
Purpose and Benefits of the Dental Provider Request Form
The Dental Provider Request Form serves multiple purposes that extend benefits to both healthcare providers and beneficiaries. It plays a crucial role in enhancing coordinated care services, allowing for better management of appointments and resource allocation.
Among the notable advantages are:
-
Streamlined appointment management for enhanced efficiency.
-
Facilitation of transport assistance and appointment reminders.
-
Improved communication within the healthcare network.
Key Features of the Dental Provider Request Form
Several key features make the Dental Provider Request Form user-friendly and effective for dental providers. Each section of the form is designed to gather specific information relevant to service requests.
Important elements include:
-
Sections for entering beneficiary information, such as names and Medicaid numbers.
-
Checkboxes for indicating various service needs, allowing for quick selections.
-
No signature is required for submission, simplifying the process.
Who Needs the Dental Provider Request Form?
The Dental Provider Request Form is essential for dental providers working with Medicaid beneficiaries in Arkansas. It is designed specifically for those providers who need to submit requests for various dental services on behalf of their patients.
Understanding eligibility is crucial, as this form is aimed at individuals who qualify for Medicaid coordinated care services. It ensures that vulnerable populations receive timely and appropriate dental care.
How to Fill Out the Dental Provider Request Form Online
Filling out the Dental Provider Request Form online is straightforward. Users should first gather necessary information, including the Medicaid number and beneficiary names, before starting the process.
Follow these steps to complete the form:
-
Access the form on the pdfFiller platform.
-
Input beneficiary details in the designated fields.
-
Select appropriate services using the provided checkboxes.
-
Review all information for accuracy and completeness.
Security and Compliance for the Dental Provider Request Form
When handling the Dental Provider Request Form, security is a top priority. The form employs advanced measures, including 256-bit encryption, to protect sensitive information.
Moreover, compliance with HIPAA and GDPR ensures that user data is managed securely. Users are encouraged to use pdfFiller's secure platform, which prioritizes privacy throughout the form submission process.
Submission Methods and Delivery
Once the Dental Provider Request Form is completed, several submission methods are available for users to choose from. Each method is designed to ensure that the form reaches the appropriate parties efficiently.
Users can opt for:
-
Online submission through pdfFiller.
-
Faxing the form to designated providers.
After submission, users can expect processing times to vary, and it’s advisable to track the status of their submission to ensure it is received and processed.
Preview of a Completed Dental Provider Request Form
Providing a visual reference can significantly aid users in understanding how to fill out the Dental Provider Request Form correctly. A sample or example of a completed form can be beneficial for this purpose.
Users can reference an image or downloadable PDF of a completed form while being made aware of common mistakes to avoid. Each section can be explained in detail using this guide.
Why Choose pdfFiller for Your Dental Provider Request Form Needs?
Choosing pdfFiller for completing the Dental Provider Request Form offers numerous advantages. The platform streamlines the form-filling process through features such as cloud-based editing and eSignature capabilities.
User experiences demonstrate successful submissions via pdfFiller, further assuring users of security, efficiency, and ease of use when managing their forms.
Get Started with Your Dental Provider Request Form Today!
Leveraging pdfFiller for the Dental Provider Request Form not only simplifies the process but also enhances the overall user experience. With user-friendly navigation and cost-effective solutions, pdfFiller is the ideal choice for filling out essential healthcare forms.
Accessing the form is easy, and users are encouraged to utilize this hassle-free method for efficient form completion and submission.
How to fill out the Dental Request Form
-
1.Access pdfFiller and find the Dental Provider Request Form by using the search bar or browsing the Healthcare Forms category.
-
2.Open the form to view its content and familiarize yourself with the available fields and checkboxes.
-
3.Before starting, collect necessary information such as the beneficiary's names, Medicaid number, date of birth, and details about the services requested.
-
4.Begin filling in the fields, clicking on each to enter information directly into the designated areas provided by pdfFiller's interface.
-
5.Utilize checkboxes for selecting specific services like appointment reminders, rescheduling, or transportation assistance.
-
6.After completing all sections, review the information entered for accuracy to ensure all required details are included.
-
7.Finalize your form by following the prompts in pdfFiller to either save, download, or submit the completed Dental Provider Request Form according to your needs.

Who is eligible to use the Dental Provider Request Form?
The Dental Provider Request Form is designed for dental providers in Arkansas seeking coordinated care for Medicaid beneficiaries. It is necessary for providers to register with Medicaid to utilize the form.
What information is required to complete the form?
You will need to provide beneficiary information such as names, Medicaid number, date of birth, and details about the requested services. Ensure you have this information ready before starting.
Are there deadlines for submitting the Dental Provider Request Form?
While there are no specific deadlines mentioned for submitting this form, it's advisable to submit it as soon as possible to avoid delays in accessing coordinated care services.
How do I submit the completed form?
Once the Dental Provider Request Form is completed on pdfFiller, you can submit it electronically or print it out for manual submission, depending on your receiving agency's requirements.
Is a signature required on the form?
The Dental Provider Request Form does not require a signature, making it simpler for providers to complete and submit on behalf of beneficiaries.
What common mistakes should I avoid when filling out the form?
Ensure all fields are filled out accurately, double-check beneficiary details, and make sure to select all relevant checkboxes for services requested to prevent processing delays.
How will I know if my form has been processed?
After submission, follow up with the appropriate dental or Medicaid office regarding the status of your request to confirm that it has been received and processed.
Related Forms







Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.