Last updated on May 2, 2026

Get the free Authorization for Disclosure of Protected Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
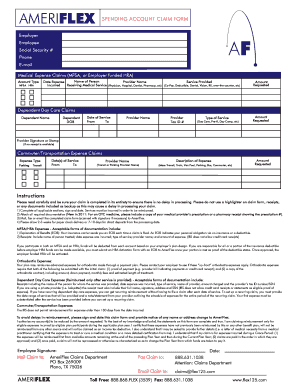
What is Health Info Release Form
The Authorization for Disclosure of Protected Health Information is a medical records release form used by patients to request access to their health information.
pdfFiller scores top ratings on review platforms
Who needs Health Info Release Form?
Explore how professionals across industries use pdfFiller.

Health Info Release Form is needed by:
-
Patients seeking access to their medical records
-
Authorized representatives of patients for health information requests
-
Healthcare providers requiring patient consent to share medical records
-
Legal professionals needing documentation for cases involving health information
-
Researchers who require patient consent for health data access
Comprehensive Guide to Health Info Release Form
What is the Authorization for Disclosure of Protected Health Information?
The Authorization for Disclosure of Protected Health Information is an essential form that allows patients at Saint Peter’s University Hospital to access their medical records. This authorization is significant as it ensures that patients maintain control over their health information, enabling them to share it with healthcare providers or other entities as needed. By understanding this authorization, patients can take proactive steps to manage their health care effectively.
Purpose and Benefits of the Authorization for Disclosure of Protected Health Information
Patients or their representatives may need to complete the authorization to access personal medical records for various reasons. This access provides numerous advantages:
-
Facilitates informed decision-making regarding treatments.
-
Supports continuity of care among different healthcare providers.
-
Empowers patients to have control over who sees their health information.
This medical records release form plays a critical role in ensuring that patients receive comprehensive care tailored to their needs.
Who Needs the Authorization for Disclosure of Protected Health Information?
The form must be filled out by specific individuals or parties, including:
-
Patients seeking their medical records.
-
Legal representatives acting on behalf of the patient in certain situations.
Understanding who requires this authorization is crucial for ensuring proper access to health information.
Eligibility Criteria for Using the Authorization for Disclosure of Protected Health Information
To submit the form successfully, certain eligibility criteria must be met:
-
Patients must be of legal age or have a guardian complete the form on their behalf.
-
Legal representatives can fill out the form under specific circumstances.
These criteria aid in complying with regulations regarding the release of health information, particularly in New Jersey.
How to Fill Out the Authorization for Disclosure of Protected Health Information Online
Filling out the authorization form online involves several key steps to ensure accuracy:
-
Access the online platform hosting the health information release form.
-
Enter the patient's name and date of birth in the designated fields.
-
Specify the type of information being requested and its intended use.
Being meticulous while completing the medical record request form will help avoid delays in processing.
Common Errors and How to Avoid Them When Submitting the Authorization for Disclosure of Protected Health Information
While filling out the authorization form, users may encounter several common errors. To mitigate these issues, consider the following tips:
-
Double-check all entered information for accuracy.
-
Ensure that the form is signed by the appropriate parties.
Recognizing these frequent mistakes can greatly enhance the submission process.
Where to Submit the Authorization for Disclosure of Protected Health Information
Submitting the authorization form can be done through various methods:
-
Online via the hospital’s designated portal.
-
Mail to the appropriate address provided on the form.
-
In-person at the hospital’s records department.
Following the correct submission method is crucial for efficient processing.
Tracking Your Submission for the Authorization for Disclosure of Protected Health Information
Once the form is submitted, patients should monitor its status by:
-
Confirming receipt through the selected submission method.
-
Checking back after the expected processing timelines for updates.
Staying informed on the status of the protected health information authorization ensures timely access to medical records.
Security and Compliance When Handling the Authorization for Disclosure of Protected Health Information
Understanding security measures is vital when handling sensitive health information. Compliance with HIPAA and maintaining data protection standards is paramount to safeguard patient records. Secure handling practices foster trust and reliability in the health information disclosure form process.
Experience Smooth Form Submission with pdfFiller
For those looking to simplify their form completion experience, pdfFiller provides an effective solution. Users can enjoy features such as editing, filling, and eSigning documents in a secure environment. Utilizing pdfFiller not only enhances ease of use but ensures that sensitive information remains protected throughout the process.
How to fill out the Health Info Release Form
-
1.Begin by accessing the Authorization for Disclosure of Protected Health Information on pdfFiller by searching for the form in the platform's search bar or navigating through the healthcare forms category.
-
2.Once you have opened the form, familiarize yourself with the layout and the fields that need to be filled out, paying particular attention to sections labeled with prompts like 'Patient Name', 'Date of Birth', and 'Home Address'.
-
3.Before filling out the form, gather all necessary information, including your medical record details, the specific type of health information you are requesting, and the relevant dates of service.
-
4.Proceed to enter your personal details in the designated fields, ensuring accuracy to avoid any delays in processing your request.
-
5.Use the checkbox options if applicable, and ensure that you indicate the purpose of the information release clearly in the provided section.
-
6.If you're completing the form as a representative, include your information and specify your relationship to the patient as required.
-
7.After entering all the necessary data, carefully review the completed form for any errors or omissions, ensuring all fields are filled and the information is correct.
-
8.Finalize your form by signing in the designated signature field and indicate the date and time to validate the authorization.
-
9.Save your completed form through pdfFiller’s saving option, and choose to download a copy for your records. You can also follow the platform's instructions to submit it directly if required.

Who is eligible to use this form?
Patients of Saint Peter's University Hospital or their authorized representatives can use this Authorization for Disclosure of Protected Health Information form to access their medical records.
Are there any deadlines for submitting this authorization?
While there are generally no strict deadlines for submitting this form, it is important to submit it promptly to ensure timely access to your needed medical records.
How can I submit the completed form?
Once the form is completed and signed, it can be submitted directly to Saint Peter's University Hospital's Records Department, either in person or via mail, as specified in their patient information guidelines.
What supporting documents are required with this form?
Typically, no additional documents are required if you are the patient. However, if a representative is filling it out, proof of the authorization relationship may need to be provided.
What are common mistakes to avoid when completing this form?
Common mistakes include omitting required fields, incorrect patient information, and not signing or dating the form, which can delay processing.
What is the processing time for requests made with this authorization?
Processing time can vary based on the volume of requests at the hospital; however, it may take up to 30 days for your request to be fulfilled.
Can I change my mind after submitting this authorization?
Yes, you can revoke the authorization in writing, but any information released prior to the revocation will still remain valid.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.