Last updated on Apr 10, 2026
Get the free Kentucky Medicaid Recipient Notification Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is kentucky medicaid recipient notification
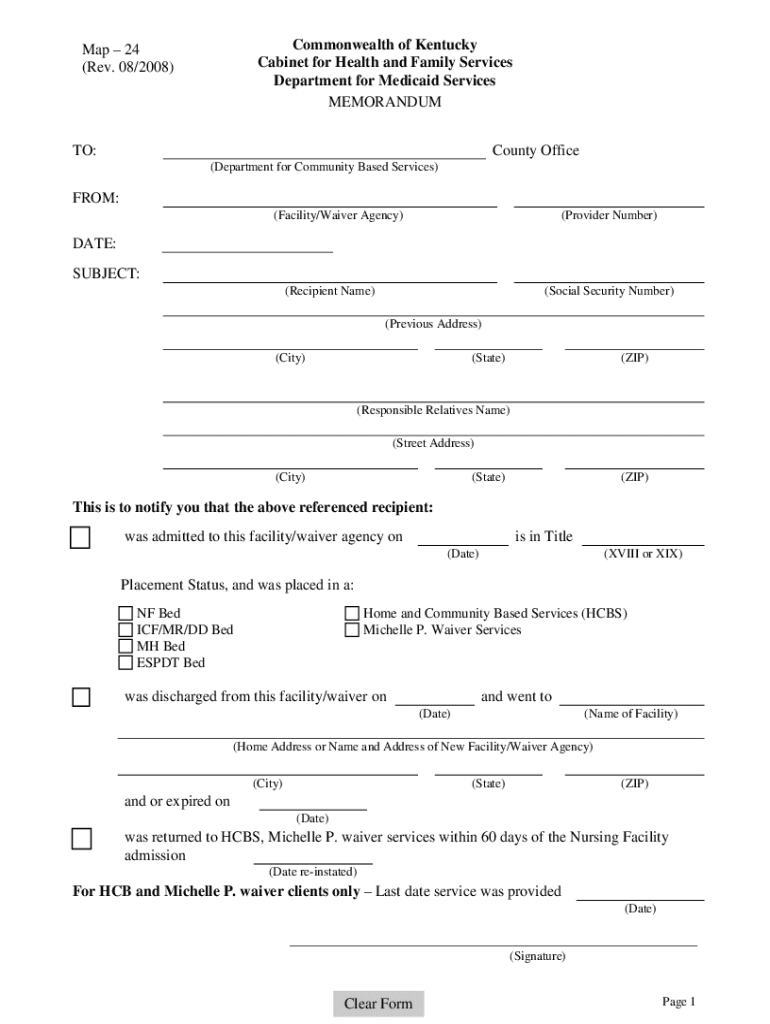
The Kentucky Medicaid Recipient Notification Form is an official document used by the Cabinet for Health and Family Services to notify county offices about Medicaid recipients' admissions, discharges, or expirations.
pdfFiller scores top ratings on review platforms
Who needs kentucky medicaid recipient notification?
Explore how professionals across industries use pdfFiller.

Kentucky medicaid recipient notification is needed by:
-
Facility administrators managing Medicaid services
-
Waiver agency representatives overseeing recipient placement
-
Health care workers involved in patient admissions and discharges
-
Social workers handling Medicaid cases
-
County health department staff monitoring Medicaid recipients
Comprehensive Guide to kentucky medicaid recipient notification
What is the Kentucky Medicaid Recipient Notification Form?
The Kentucky Medicaid Recipient Notification Form is a crucial document utilized by the Cabinet for Health and Family Services to inform county offices about Medicaid recipients. This form addresses the admission, discharge, or expiration of individuals receiving Medicaid services across various facilities or waiver programs. Facilities and waiver agencies primarily use this Medicaid recipient form to ensure timely and accurate communication.
Purpose and Benefits of the Kentucky Medicaid Recipient Notification Form
This health and family services form plays an essential role in maintaining compliance with Medicaid regulations. Timely notifications help recipients and county offices stay informed about important changes related to admissions and discharges. As a result, the form facilitates better communication, minimizing gaps in care and improving service delivery.
Key Features of the Kentucky Medicaid Recipient Notification Form
The Kentucky Medicaid Recipient Notification Form includes several important elements that users should be aware of:
-
Fillable fields for Recipient Name, Social Security Number, and Date
-
Check boxes indicating various placement statuses
-
Clear instructions for form completion
These features help ensure that the form is filled out accurately and comprehensively.
Who Needs the Kentucky Medicaid Recipient Notification Form?
This form is primarily required by various types of facilities and agencies, including:
-
Nursing homes
-
Assisted living facilities
-
Waiver agencies providing home- and community-based services
Medicaid recipients may be affected by these notifications, making it vital for the relevant parties to complete the form correctly and on time.
How to Fill Out the Kentucky Medicaid Recipient Notification Form Online (Step-by-Step)
To complete the Kentucky Medicaid Recipient Notification Form online using pdfFiller, follow these step-by-step instructions:
-
Access the form through pdfFiller.
-
Fill in the required fields such as Recipient Name and Social Security Number.
-
Select the appropriate placement status checkboxes.
-
Review the information for accuracy.
-
Sign the document if required.
-
Submit the form according to the preferred method.
This digital process allows for efficient completion and submission of the health and family services form.
Common Errors and How to Avoid Them
When completing the Kentucky Medicaid Recipient Notification Form, users may encounter some common errors, including:
-
Omitting the required signatures
-
Entering incorrect Social Security numbers
-
Failing to check relevant placement status boxes
To ensure accuracy, double-check all entries before submission and consider using tools that facilitate accurate data entry.
Submission Methods for the Kentucky Medicaid Recipient Notification Form
Once the form is completed, users can submit it through various methods:
-
Online submission via pdfFiller
-
Mailing to the appropriate county office
-
Faxing the completed form
It is essential to be aware of delivery options and potential deadlines to prevent any disruptions in services.
Security and Compliance for the Kentucky Medicaid Recipient Notification Form
When utilizing pdfFiller for the Kentucky Medicaid Recipient Notification Form, users can have peace of mind regarding security. pdfFiller employs 256-bit encryption, ensuring all sensitive information is securely processed. Furthermore, the platform adheres to HIPAA and GDPR regulations, reinforcing its commitment to compliance and the protection of users’ data.
Tracking Your Submission and What Happens Next
After submitting the form, users can track their submission status by:
-
Accessing the submission portal on pdfFiller
-
Contacting the relevant county office for updates
Recipients can expect notifications regarding the outcome of their submissions and may need to engage in follow-up actions as advised.
Get Started with the Kentucky Medicaid Recipient Notification Form Using pdfFiller
pdfFiller offers an intuitive platform to create, edit, and securely submit the Kentucky Medicaid Recipient Notification Form. With a focus on ease of use, users can manage their documents efficiently, ensuring all requirements are met seamlessly. Try pdfFiller today to experience a streamlined approach to form handling.
How to fill out the kentucky medicaid recipient notification
-
1.To access the Kentucky Medicaid Recipient Notification Form on pdfFiller, visit the pdfFiller website and search for the form by its name.
-
2.Once you have located the form, click on it to open the interactive PDF editor where you can begin filling it out.
-
3.Gather all necessary information before starting, including the recipient's full name, social security number, admission and discharge dates, and facility details.
-
4.Use pdfFiller's interface to navigate through the form. Click on each field to enter information. Utilize the provided fillable spaces for the recipient's name, social security number, dates, and signature.
-
5.Ensure to check the appropriate placement status checkboxes as per the recipient's situation. Follow the explicit instructions provided on the form for clarity.
-
6.After completing the form, carefully review all entries for accuracy. Check that the required fields are filled and all necessary information is provided before proceeding.
-
7.Once you are satisfied with the filled form, save your entry. You can download it in various formats or proceed to submit it directly through pdfFiller.
-
8.Remember that the form must be signed by an authorized representative from your facility or waiver agency before submission.

Who is eligible to use the Kentucky Medicaid Recipient Notification Form?
This form is intended for facilities and waiver agencies that manage Medicaid recipients. It must be completed by authorized individuals responsible for notifying county offices about any admission, discharge, or changes in status.
What is the deadline for submitting the Kentucky Medicaid Recipient Notification Form?
It's essential to submit this form as soon as there is any change in the status of a Medicaid recipient. Prompt submission helps ensure that county offices have the most current information to manage services effectively.
How should the Kentucky Medicaid Recipient Notification Form be submitted?
The form can be submitted electronically via pdfFiller or printed and sent directly to the appropriate county office by mail. Be sure to follow any specific submission guidelines included with the form.
Are there any required supporting documents when submitting this form?
While the form itself does not require additional documents, having the recipient's records, such as identification and previous service documentation, on hand may facilitate accurate completion.
What common mistakes should I avoid when filling out the form?
Common mistakes include not providing complete information, missing signatures, and overlooking checkboxes for placement status. Double-check all entries to prevent delays in processing.
How long does it take to process the Kentucky Medicaid Recipient Notification Form?
Processing times can vary depending on the county office. Typically, forms are processed within a few business days. Contact your local office for more specific timelines.
Can I edit the Kentucky Medicaid Recipient Notification Form after submission?
Once submitted, the form usually cannot be edited. If necessary, submit a new form with the correct information or contact your county office for assistance regarding changes.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.