Last updated on Apr 10, 2026
Get the free Open Enrollment Medical Plan Change Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is open enrollment medical plan
The Open Enrollment Medical Plan Change Request Form is a healthcare document used by employers to request changes to their employees' medical plans during the renewal period.
pdfFiller scores top ratings on review platforms
Who needs open enrollment medical plan?
Explore how professionals across industries use pdfFiller.

Open enrollment medical plan is needed by:
-
Employers seeking to update employee medical plans
-
HR professionals managing employee benefits
-
Employees participating in open enrollment
-
Dependents covered under group plans
-
Insurance brokers facilitating plan changes
-
Benefits administrators handling documentation
Comprehensive Guide to open enrollment medical plan
What is the Open Enrollment Medical Plan Change Request Form?
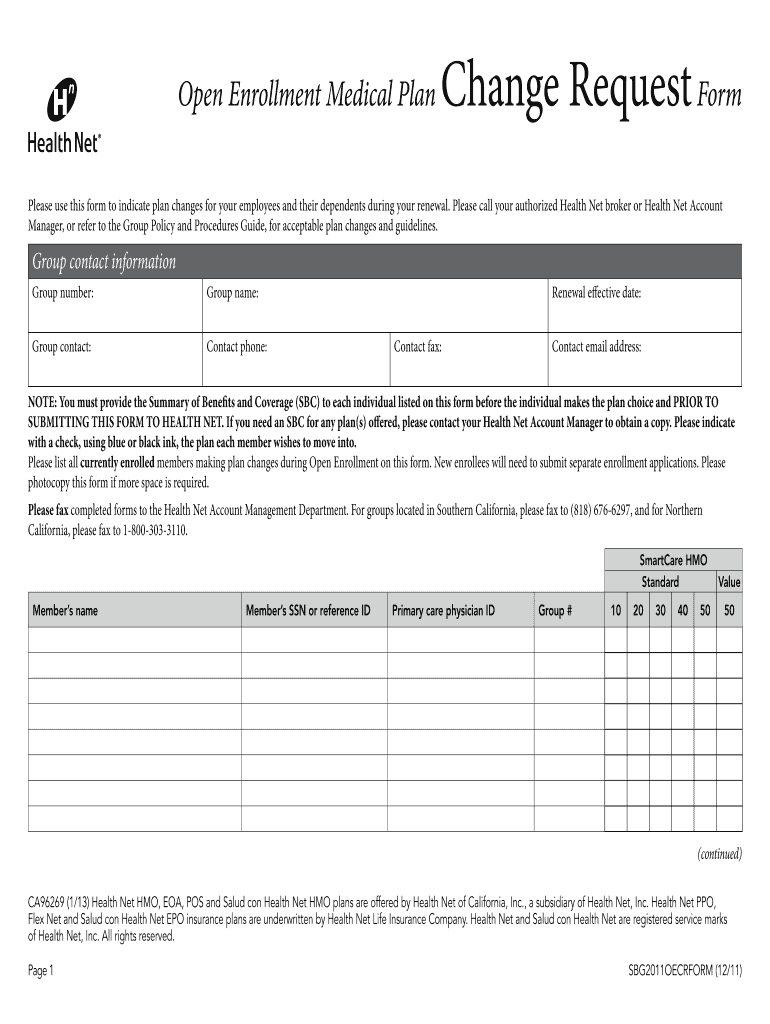
The Open Enrollment Medical Plan Change Request Form serves a crucial role in managing medical plan enrollments and changes. Employers utilize this form to communicate necessary modifications during open enrollment, ensuring all employees understand their options for coverage. Key fields required on the form include group contact information and detailed member data to accurately reflect each participant's needs.
This form is specifically relevant for processes in California, integrating terms like the California Open Enrollment Form and the Health Net Medical Plan Change Form to streamline communication between employers and employees.
Purpose and Benefits of the Open Enrollment Medical Plan Change Request Form
This document presents significant benefits for both employers and employees alike. It simplifies plan modifications for employees and their dependents, providing a structured way to adjust coverage during the open enrollment period. Additionally, it requires a Summary of Benefits and Coverage (SBC) to ensure that employees have a clear understanding of the changes being made.
By facilitating these changes, the form not only aids in compliance but also enhances employee satisfaction with health coverage options.
Key Features of the Open Enrollment Medical Plan Change Request Form
The form comes equipped with key features such as fillable fields and checkboxes for selecting various plan options. Clear instructions guide users in completing the required information efficiently. Security measures are in place to protect sensitive information submitted through the form, ensuring a safe transaction process.
-
Fillable fields for user convenience
-
Checkboxes to facilitate plan choice
-
Explicit instructions for accurate completion
-
Security features to safeguard personal data
Who Needs the Open Enrollment Medical Plan Change Request Form?
This form is essential for employers or designated officers who manage employee health plans. Employees wishing to change their health coverage or add dependents during the open enrollment period also need to complete this form. Adhering to the form's requirements is vital for ensuring that all coverage modifications are processed correctly and promptly.
When to Submit the Open Enrollment Medical Plan Change Request Form
Submission of the form should occur during the designated open enrollment period. Employers and employees must be mindful of specific deadlines outlined for California to avoid potential disruptions in coverage. Late filings or failure to submit the form can result in denial of coverage changes, emphasizing the importance of timely action.
How to Fill Out the Open Enrollment Medical Plan Change Request Form Online (Step-by-Step)
Filling out the form online via pdfFiller is a straightforward process. Follow these steps to ensure accuracy:
-
Gather necessary information, including group and member details.
-
Access pdfFiller and upload the form template.
-
Complete each fillable field meticulously.
-
Select appropriate plan options from available checkboxes.
-
Review all information for accuracy before submission.
Completing these steps efficiently will help in submitting a valid request for changes to medical plans.
Review and Validation Checklist
Before submitting the form, consider using a checklist to validate crucial fields. This checklist can prevent common errors that may arise:
-
Check group number for accuracy
-
Ensure the effective date is correct
-
Confirm that all members' details are complete
Careful review using this checklist can significantly decrease the chance of submission errors.
Submission and Delivery Methods for the Open Enrollment Medical Plan Change Request Form
Completed forms can be submitted through various methods, including faxing to designated numbers based on specific regions in California. It is important to know that additional documentation, such as the Summary of Benefits and Coverage (SBC), may need to be attached to the form. Ensuring all required documents are included will aid in a smooth processing experience.
What Happens After You Submit the Open Enrollment Medical Plan Change Request Form?
After submission, the processing time for the changes can vary. Users can confirm their submission and check the status of their request through provided channels. Staying informed about the progress of your submission is crucial for peace of mind and timely responses regarding your health plan changes.
Experience Seamless Form Filling with pdfFiller
pdfFiller simplifies the process of completing the Open Enrollment Medical Plan Change Request Form. This platform provides numerous security measures to protect sensitive data throughout the form filling and submission process. Users are encouraged to take advantage of pdfFiller's features to create, edit, and submit forms effectively, ensuring a hassle-free experience.
How to fill out the open enrollment medical plan
-
1.Access the Open Enrollment Medical Plan Change Request Form on pdfFiller by searching its name in the platform's search bar.
-
2.Once the form is open, familiarize yourself with the various sections and fields available for input.
-
3.Gather the necessary information, including group contact details, individual member information, and renewal dates prior to filling out the form.
-
4.Begin by entering the 'Group number' and 'Group name' in the designated fields.
-
5.Fill in the 'Renewal effective date' using the date picker or by typing in the format required.
-
6.Select the applicable medical plan options using the checkboxes provided, ensuring you choose the correct options for each member.
-
7.Review all populated fields for accuracy and completeness before finalizing the document.
-
8.Utilize pdfFiller's review tools to check for any errors or missing information on the form.
-
9.Once you are satisfied with the completed form, save it to your account on pdfFiller for future reference.
-
10.To submit, either fax the form directly to Health Net’s Account Management department or download it for personal submission.

Who is eligible to use the Open Enrollment Medical Plan Change Request Form?
Employers, HR professionals, and employees enrolled in group plans during the designated open enrollment period can utilize this form to request changes to their medical coverage.
What details are required to complete the form?
You will need to provide group contact information, member details, and any changes to the medical plans selected, including the renewal effective date.
What is the deadline for submitting the form?
Typically, the form must be submitted during the designated open enrollment period outlined by your insurance provider, so it’s essential to check specific deadlines with Health Net.
How should I submit the completed form?
The completed form should be faxed to Health Net’s Account Management, using the designated fax numbers for Southern and Northern California or mailed if preferred.
What common mistakes should I avoid when filling out the form?
Ensure that all fields are accurately completed and all necessary checkboxes are selected, as incomplete entries may delay processing.
Is there a fee associated with submitting the Open Enrollment Medical Plan Change Request Form?
There are typically no fees for submitting this form, but it is advisable to confirm with Health Net if any specific fees apply.
Do I need any supporting documents along with this form?
Yes, the form must be accompanied by a Summary of Benefits and Coverage (SBC) for each individual listed, as this is critical for processing.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.