Last updated on Apr 19, 2016
Get the free Prescription Reimbursement Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Reimbursement Request Form
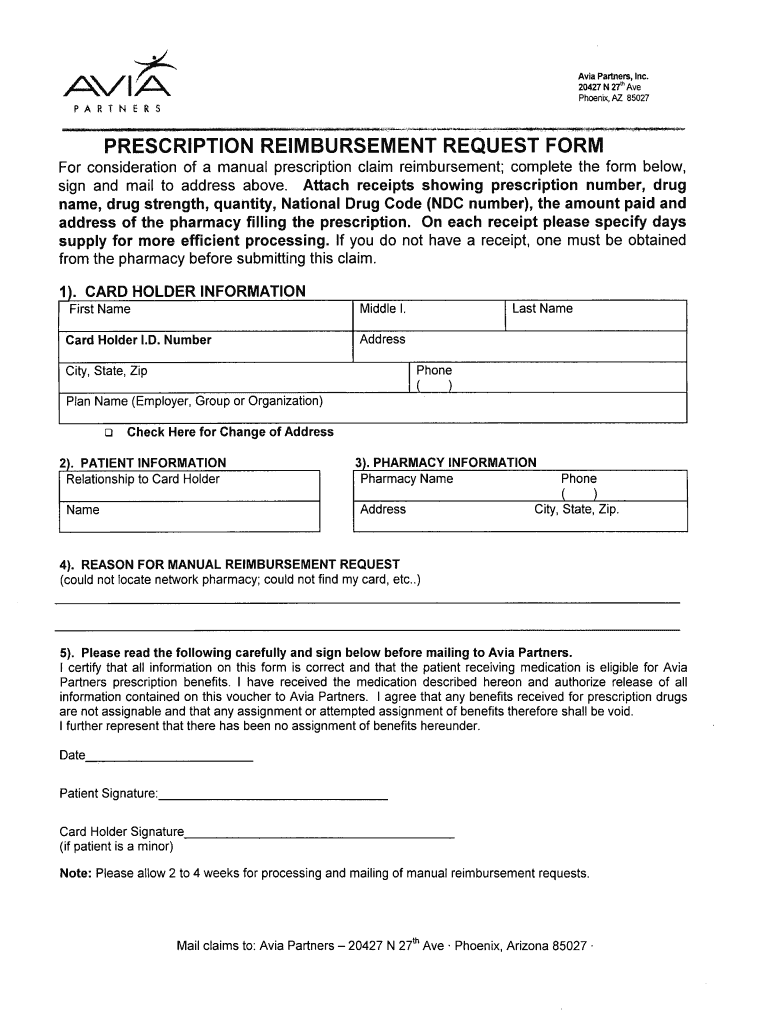
The Prescription Reimbursement Request Form is a medical billing document used by patients to request manual reimbursement for prescription claims.
pdfFiller scores top ratings on review platforms
Who needs Reimbursement Request Form?
Explore how professionals across industries use pdfFiller.

Reimbursement Request Form is needed by:
-
Patients seeking reimbursement for prescription costs
-
Card holders involved in health insurance plans
-
Pharmacies providing necessary prescription documentation
-
Individuals managing medical billing and claims
-
Healthcare providers requiring prescription records
Comprehensive Guide to Reimbursement Request Form
What is the Prescription Reimbursement Request Form?
The Prescription Reimbursement Request Form serves as a critical document for patients seeking to obtain reimbursement for their prescription medications. Patients can use this form to submit claims to Avia Partners, ensuring they receive compensation for out-of-pocket expenses. Additionally, it is essential to provide information for both the patient and the card holder, optimizing the process for claims management.
Purpose and Benefits of Using the Prescription Reimbursement Request Form
Utilizing the Prescription Reimbursement Request Form offers numerous advantages. Foremost, it allows patients to reclaim funds spent on prescription medications, providing significant financial relief. Submitting a reimbursement request helps ensure that patients can manage their healthcare costs more effectively. To maximize the chances of a successful claim, it is crucial to compile accurate receipts and associated documentation.
Who Needs the Prescription Reimbursement Request Form?
The target audience for this form primarily includes patients who have purchased medications. Card holders, along with caregivers or guardians assisting patients, may also require this form. In Arizona, specific eligibility criteria apply, ensuring that only qualifying individuals can utilize the request form for reimbursement.
How to Fill Out the Prescription Reimbursement Request Form: Step-by-Step Guide
Filling out the Prescription Reimbursement Request Form can be accomplished by following these simple steps:
-
Start by entering your personal information in the designated fields.
-
Provide the card holder’s details, ensuring accuracy in both sections.
-
Insert prescription details, including the pharmacy's name and prescription number.
-
Attach relevant receipts that clearly show the amount paid for medications.
-
Review the form for any common errors before signing.
Avoid mistakes by double-checking all entries and ensuring all required sections are completed.
Required Documents and Supporting Materials for Your Request
To successfully submit your request, gather and organize the following required documents:
-
Itemized receipts from the pharmacy showing your prescription purchases.
-
Prescription details, including the prescription number and medication information.
-
Any additional forms or information specified by Avia Partners.
Maintaining meticulous records of these documents is vital for tracking your claim and ensuring smooth processing.
Submission Methods for the Prescription Reimbursement Request Form
Once the form is filled out, you can submit it through various channels:
-
Mail the completed form to the designated address in Phoenix, Arizona.
-
Utilize electronic submission options if available from your insurance provider.
It is crucial to track your submissions to confirm that your request is received and to be aware of any potential fees associated with the submission process.
What Happens After You Submit the Prescription Reimbursement Request Form?
After submission, Avia Partners will review your request. The typical timeline for processing reimbursement claims varies, but you can typically expect confirmation of receipt within a few business days. Throughout this period, you can track the status of your claim to ensure timely resolution.
Common Reasons for Rejection and How to Avoid Them
Several factors can lead to the rejection of your reimbursement request. Common mistakes include:
-
Incomplete or inaccurate information on the form.
-
Failure to attach necessary supporting documents.
-
Missing signatures from the patient or card holder.
To avoid these pitfalls, ensure that your submission is thorough and that all sections of the form are filled out correctly.
Why Use pdfFiller for Your Prescription Reimbursement Request Form?
Leveraging pdfFiller for your Prescription Reimbursement Request Form provides several key benefits. This platform offers intuitive features such as eSigning, form filling, and document management, making the process straightforward and user-friendly. Security measures are paramount, with pdfFiller being HIPAA compliant, ensuring your sensitive information is protected. User testimonials highlight the reliability and ease of using pdfFiller for this important document.
Start Filling Out Your Prescription Reimbursement Request Form Today!
Begin the process of reclaiming your prescription costs by accessing the form on pdfFiller’s website. The platform offers exceptional tools for filling and submitting your request securely. Experience the simplicity and safety of using pdfFiller for managing your healthcare documents.
How to fill out the Reimbursement Request Form
-
1.To begin, access the Prescription Reimbursement Request Form on pdfFiller by searching for its name in the search bar or navigating through the Healthcare Forms category.
-
2.Once the form opens, familiarize yourself with the layout, noting the fields designated for patient and card holder information.
-
3.Before starting to fill out the form, gather necessary information, including receipts with prescription numbers, drug details, and amounts paid. Ensure that all information is accurate.
-
4.Begin filling the form by clicking on the blank fields. Type the required information into the designated sections using pdfFiller’s user-friendly interface.
-
5.Use the provided tabs or buttons to navigate through each section while ensuring that you complete all mandatory fields, including checkboxes indicating understanding of terms.
-
6.Once all information is filled, review the entire form carefully. Ensure accuracy and completeness to avoid processing delays.
-
7.Finalize the form by adding your signature in the required field. You can sign digitally using pdfFiller or by uploading a scanned signature.
-
8.To save or download the completed form, click the 'Save' button, then choose the preferred file format. You may also opt to directly submit the form via pdfFiller if that option is available.

Who is eligible to submit the Prescription Reimbursement Request Form?
Patients and card holders who have incurred prescription expenses are eligible to submit this form for reimbursement claims. Ensure you have the necessary receipts and documentation.
What documents are required to complete the form?
To complete the Prescription Reimbursement Request Form, you need to attach receipts including the prescription number, drug details, and the total amount paid. Accurate details are crucial for processing.
How do I submit the completed form?
After filling out the form, you can either mail it to the provided address in Phoenix, Arizona, or, if using pdfFiller, submit it electronically if that option is available.
What are common mistakes to avoid while filling the form?
Common mistakes include missing required signatures, failing to attach necessary receipts, and entering inaccurate or incomplete information. Always double-check your form before submission.
How long does it take to process the reimbursement request?
Processing times can vary, but generally expect a response within 4-6 weeks after submission. Be sure to submit the form early to account for potential delays.
Can I amend my submission after it’s been mailed?
Once submitted, amending the form is not guaranteed. If you realize there is an error after submission, contact the billing department immediately for possible corrective procedures.
Related Forms



Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.