
Get the free Authorization for Examination or Treatment
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
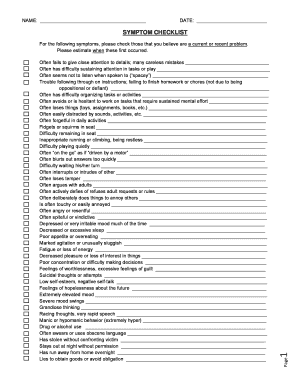
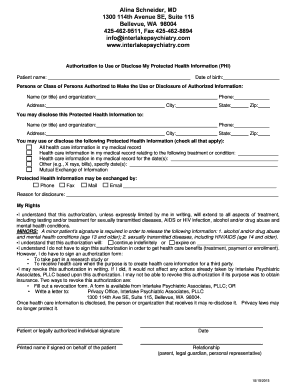
What is Medical Authorization Form
The Authorization for Examination or Treatment is a medical consent form used by patients to grant permission for medical examinations or treatments.
pdfFiller scores top ratings on review platforms
Who needs Medical Authorization Form?
Explore how professionals across industries use pdfFiller.

Medical Authorization Form is needed by:
-
Patients seeking medical examinations
-
Authorized representatives providing consent
-
Healthcare providers conducting evaluations
-
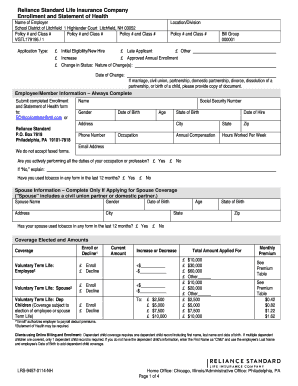
Employers requiring work-related physicals
-
Substance abuse testing administrators
How to fill out the Medical Authorization Form
-
1.To access the Authorization for Examination or Treatment form on pdfFiller, navigate to the website and use the search bar to find the form by typing its name.
-
2.Once the form appears, click on it to open in the pdfFiller editor interface, where you can begin filling it in.
-
3.Before starting, gather all necessary information such as your personal information and any details about the specific examination or treatment type required.
-
4.Begin by entering your name and personal details in the designated fields at the top of the form.
-
5.For each examination type, check the appropriate boxes to indicate which evaluations you are authorizing.
-
6.If applicable, fill in the section for the authorized person's details, ensuring it is clear who is granting consent.
-
7.Once you have completed filling all required fields, review the entire form for accuracy and completeness, ensuring that no sections are left blank.
-
8.After verification, you can finalize the form by clicking on the 'Save' button to store it on your pdfFiller account.
-
9.To download a copy of the completed form, select the download option, or choose to submit it directly if required by your healthcare provider.

Who is eligible to use the Authorization for Examination or Treatment form?
Any patient seeking permission for medical examinations or treatments can use this form. Additionally, an authorized representative can fill out the form on behalf of the patient.
What types of examinations does this form cover?
The form covers a variety of medical evaluations, including work-related physicals and substance abuse testing. It can be adapted to suit various healthcare situations requiring patient consent.
How do I submit the completed Authorization for Examination or Treatment form?
After completing the form on pdfFiller, you can either download it for personal records or submit it electronically to your healthcare provider, depending on their submission requirements.
Are there any documents I need to provide along with the form?
Usually, no additional documents are required, but you might want to have identification or supplementary medical records handy in case your provider requests them.
What should I do if I make a mistake while filling out the form?
If you make a mistake, use the edit option in pdfFiller to correct it. Ensure all information is accurate before saving or submitting the form to avoid processing delays.
Are there deadlines for submitting this form?
Deadlines may vary based on the healthcare provider's requirements. It is advisable to complete and submit the form as soon as possible to avoid any disruptions in receiving medical care.
How long does processing the Authorization for Examination or Treatment take?
The processing time typically depends on the healthcare provider's office. Generally, expect a response or confirmation within a few business days after submission.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.