Last updated on Apr 18, 2026

Get the free Medicare Part B Drug Prior Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medicare part b drug
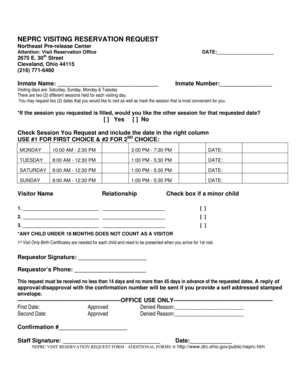
The Medicare Part B Drug Prior Authorization Form is a healthcare document used by prescribers to request prior authorization for specific Part B drugs under the Medicare program.
pdfFiller scores top ratings on review platforms
Who needs medicare part b drug?
Explore how professionals across industries use pdfFiller.

Medicare part b drug is needed by:
-
Healthcare providers managing Medicare patients
-
Pharmacies processing Medicare prescriptions
-
Insurance companies reviewing drug requests
-
Medicare beneficiaries requiring medication
-
Medical billing professionals handling prior authorizations
Comprehensive Guide to medicare part b drug
What is the Medicare Part B Drug Prior Authorization Form?
The Medicare Part B Drug Prior Authorization Form serves as a key document in healthcare, enabling healthcare providers to request prior authorization for specific Part B drugs. This form is crucial for ensuring that medications are covered under Medicare, allowing patients to receive necessary treatments without facing unforeseen costs. It collects vital information such as patient details, prescriber information, and specific medication requests.
Purpose and Benefits of the Medicare Part B Drug Prior Authorization Form
This form benefits both healthcare providers and patients by facilitating medication coverage approval. It ensures that prescribed treatments are cost-effective and appropriate for patients’ health conditions. By obtaining prior authorization, healthcare providers can enhance patient outcomes, reducing the likelihood of medication-related complications.
Key Features of the Medicare Part B Drug Prior Authorization Form
The form includes several fillable fields necessary for its completion. These fields typically encompass:
-
Patient information, such as name and ID number
-
Details about the requested medication
-
Clinical information relevant to the request
Additionally, it contains checkboxes for specific queries and explicit instructions for proper completion. The prescriber’s signature is a critical component, along with any necessary additional documentation to ensure a successful submission.
Who Needs the Medicare Part B Drug Prior Authorization Form?
This form is essential for various healthcare providers, including physicians and specialists recommending specific medications. Patient eligibility is determined by their Medicare enrollment and the specific criteria required for the requested drugs. Common medications needing prior authorization often include high-cost treatments or those used for chronic conditions.
How to Fill Out the Medicare Part B Drug Prior Authorization Form Online
To complete the form digitally using pdfFiller, follow these steps:
-
Navigate to the pdfFiller site and access the form.
-
Fill in all applicable fields accurately, including patient and medication details.
-
Review the form to ensure all necessary information is included.
-
Use the validation checklist provided by pdfFiller before submission.
Ensuring accuracy in completion helps avoid delays in processing the authorization request.
Submission Methods and Delivery for the Medicare Part B Drug Prior Authorization Form
There are multiple ways to submit the completed form. The available methods include online submission through pdfFiller, or via fax. To ensure successful submission, it is essential to follow the instructions explicitly and track confirmation after sending. Be mindful of submission deadlines and the expected processing times for approvals.
Common Errors and How to Avoid Them
Several common mistakes can occur during the completion of the form, such as missing signatures or incomplete fields. To minimize errors, consider these tips:
-
Double-check all entries for accuracy before submission.
-
Attach any required supporting documents to prevent potential delays.
Taking these precautions can greatly enhance the likelihood of a successful submission.
Security and Compliance for the Medicare Part B Drug Prior Authorization Form
Handling sensitive patient information demands a strong focus on data protection. pdfFiller implements numerous security measures, including 256-bit encryption, to uphold high standards of compliance with HIPAA and GDPR regulations. Utilizing pdfFiller for managing this form ensures that patient data remains secure throughout the process.
Sample or Example of a Completed Medicare Part B Drug Prior Authorization Form
A completed example of the Medicare Part B Drug Prior Authorization Form illustrates how it should be filled out. Each section includes essential details like patient identifiers and medication specifics. This example serves as a valuable guide for individuals preparing their own submissions, clarifying expectations for each part of the form.
Maximize Your Medicare Prior Authorization Experience with pdfFiller
Employing pdfFiller offers significant advantages for form completion and management. The platform’s user-friendly tools streamline the process of creating, filling, and eSigning documents. It also enhances security, allowing users to manage sensitive forms efficiently while ensuring compliance with relevant regulations.
How to fill out the medicare part b drug
-
1.To access the Medicare Part B Drug Prior Authorization Form on pdfFiller, visit the website and use the search feature to locate the specific form by name.
-
2.Once you have opened the form, familiarize yourself with the fillable fields including 'Name:', 'ID Number:', and 'Date of Birth.'
-
3.Gather all necessary information such as patient details, prescriber information, and clinical data before starting to fill out the form.
-
4.Begin filling out the form by entering the member's personal information in the appropriate fields, ensuring accuracy to avoid delays.
-
5.Next, input the medication requested, including specifics like ‘Drug Name:’, ‘Directions/SIG:’, and ‘ICD-9 Code:’ if applicable.
-
6.Remember to check relevant boxes, such as whether the medication is being used as part of an investigational trial.
-
7.Once you have completed all sections, take a moment to review the information for any errors or omissions.
-
8.Finalize the form by adding the prescriber’s signature in the designated area and ensuring all required fields are filled.
-
9.After reviewing, you can save your work on pdfFiller, either downloading the document directly or submitting it electronically as per the instructions provided.
-
10.If submitting via fax, print the document and fax it to the number indicated on the form, typically located under the logo.

Who is eligible to use the Medicare Part B Drug Prior Authorization Form?
This form is designed for healthcare providers, specifically prescribers enrolled in Medicare, who need to request prior authorization for specific medications for their patients.
Is there a deadline for submitting the prior authorization request?
While specific deadlines can vary, it is generally recommended to submit the form as soon as possible to avoid delays in medication approval, especially for time-sensitive treatments.
What are the submission methods for this form?
The completed Medicare Part B Drug Prior Authorization Form can be submitted via fax, as indicated in the form instructions. Ensure to retain a copy for your records.
What supporting documents are required with this form?
Typically, supporting documents include the patient's medical history related to the medication requested and any relevant clinical information that justifies the need for prior authorization.
What are common mistakes to avoid when filling out the form?
Ensure all fields are filled out completely and accurately, especially signature lines. Common mistakes include missing signatures or not providing full patient information.
What is the typical processing time for prior authorization requests?
Processing times can vary, but it usually takes several business days. Check with the specific insurance provider for their typical turnaround times.
What happens if the prior authorization is denied?
If denied, the prescriber will receive a notification outlining the reasons for denial. They can appeal the decision by providing additional information or documentation.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.