Last updated on Apr 10, 2026

Get the free Patient Assistance Program Application
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
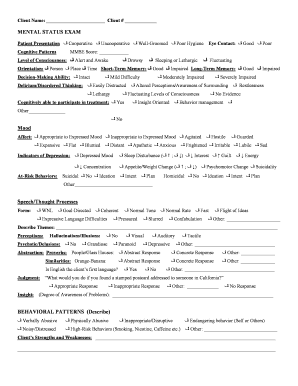
What is patient assistance program application
The Patient Assistance Program Application is a healthcare form used by patients or their legal guardians to apply for financial assistance for prescription medications.
pdfFiller scores top ratings on review platforms
Who needs patient assistance program application?
Explore how professionals across industries use pdfFiller.

Patient assistance program application is needed by:
-
Patients seeking medication financial aid
-
Legal guardians applying for assistance on behalf of patients
-
Attending physicians verifying patient diagnoses
-
Healthcare providers assisting patients with applications
-
Pharmaceutical companies offering patient assistance programs
Comprehensive Guide to patient assistance program application
What is the Patient Assistance Program Application?
The Patient Assistance Program Application is a crucial tool used by patients or their legal guardians to seek financial aid for needed prescription medications. This application serves its purpose by helping individuals navigate financial barriers that may hinder their access to essential drugs. By utilizing the patient assistance program application, applicants can potentially secure vital medication support, making healthcare more attainable for those in need.
Why Use the Patient Assistance Program Application?
Applying for the Patient Assistance Program offers various benefits, primarily financial relief for patients facing economic challenges. This application can significantly facilitate access to necessary medications, ensuring patients receive the treatment they require without overwhelming financial burden. By leveraging this healthcare financial aid, individuals can better manage their health while alleviating the stress associated with medication costs.
Who Needs to Complete the Patient Assistance Program Application?
Completion of the Patient Assistance Program Application is essential for various parties, including patients or their legal guardians, as well as attending physicians. Each role has specific responsibilities in the application process. Patients or guardians provide personal and financial details, while physicians are tasked with certifying the medical need for medication. This collaborative approach ensures a comprehensive application for assistance.
Eligibility Criteria for the Patient Assistance Program Application
To qualify for the Patient Assistance Program, applicants must meet certain eligibility criteria. These requirements typically include:
-
Gross monthly household income that falls within defined limits.
-
Proof of a recent medical diagnosis related to the prescription needed.
-
Current enrollment in Medicare or proof of lack of insurance coverage.
Understanding these guidelines can facilitate accurate completion of the application and enhance the chance of approval.
How to Fill Out the Patient Assistance Program Application Online (Step-by-Step)
Filling out the Patient Assistance Program Application online can be straightforward if you follow these steps:
-
Begin with your personal information, including name and contact details.
-
Provide your household income information accurately.
-
Submit the physician's certification, ensuring they complete their section of the form.
Completing these sections will help ensure your application is properly submitted for review.
Field-by-Field Instructions for the Patient Assistance Program Application
Each field in the Patient Assistance Program Application requires careful attention to detail. Important fields include:
-
Patient's first and last name.
-
Household income verification.
-
Insurance enrollment status details.
Avoid common errors such as incomplete fields or inaccuracies in income reporting, which can delay your application process.
Submission Process for the Patient Assistance Program Application
Submitting your Patient Assistance Program Application can be done easily through various methods. Options include:
-
Online submission via pdfFiller.
-
Tracking your application status through the provided submission portal.
Understanding the submission process is essential to ensure that your application is received and processed efficiently.
Security and Compliance for the Patient Assistance Program Application
When handling sensitive medical information, security, and compliance are paramount. The Patient Assistance Program Application process incorporates strong data protection measures to safeguard your personal information. pdfFiller ensures compliance with privacy standards and implements 256-bit encryption to protect user data during submission, aligning with HIPAA regulations.
Sample Patient Assistance Program Application
To assist users in completing the application, a visual or downloadable sample application is available. This resource includes:
-
An example of a completed Patient Assistance Program Application.
-
A detailed overview of the necessary fields and required documentation.
Utilizing this sample can clarify what is expected in each section of the application, improving accuracy and completeness.
Empowering Patients with pdfFiller: Streamline Your Application Process
pdfFiller simplifies the lengthy application process with robust features designed to assist users. These include options to edit documents, eSign applications, and manage all necessary paperwork in one central location. By leveraging these functionalities, users can effectively complete their Patient Assistance Program Application, ensuring a smoother experience.
How to fill out the patient assistance program application
-
1.Access the Patient Assistance Program Application on pdfFiller by searching for the form name in the search bar or by browsing the healthcare forms category.
-
2.Open the form in the pdfFiller interface where you can view all fillable fields.
-
3.Gather the necessary information before starting. This includes personal details of the patient, household income amounts, and Medicare Part D enrollment status.
-
4.Begin filling in the patient’s personal information including first name, last name, address, city, state, zip code, phone number, and birth date in the designated fields.
-
5.Fill in the Medicare Social Security number and any additional identification numbers required like ID# or Alien Registration number.
-
6.Provide the gross monthly household income of the applicant in the specified field.
-
7.Navigate to the section where the attending physician's information is needed, and ensure to include their diagnosis information and certification.
-
8.Sign and date the form in the designated areas for both the patient or legal guardian and the attending physician.
-
9.Before finalizing, review all filled fields for accuracy and completeness.
-
10.Once all entries are confirmed, utilize the save or download options available on pdfFiller to keep a copy of the completed form.
-
11.Consider submitting the form directly through pdfFiller, if submission options allow, or save it for print submission as required.

Who is eligible to use the Patient Assistance Program Application?
Patients or their legal guardians are eligible to use the Patient Assistance Program Application if they are seeking financial assistance for prescription medications.
Are there deadlines for submitting the application?
It's important to check specific deadlines as they may vary by program or provider. Typically, applications should be submitted as soon as financial assistance is needed.
How can I submit the completed form?
The completed form can be submitted electronically via pdfFiller or printed out for submission via mail or in person to the relevant organization.
What supporting documents are required with the application?
Supporting documents may include proof of income, Medicare Part D enrollment confirmation, and a statement from the attending physician confirming the diagnosis and need for medication.
What common mistakes should I avoid while filling out the form?
Common mistakes include leaving fields blank, incorrect entry of personal information, and failing to obtain necessary signatures from both the patient and attending physician.
How long does it take to process the application?
Processing times can vary widely depending on the organization. Generally, applicants can expect a response within a few weeks.
What if I encounter issues while filling out the form on pdfFiller?
If you encounter issues, you can consult pdfFiller’s help resources or contact their customer support for assistance with the form.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.