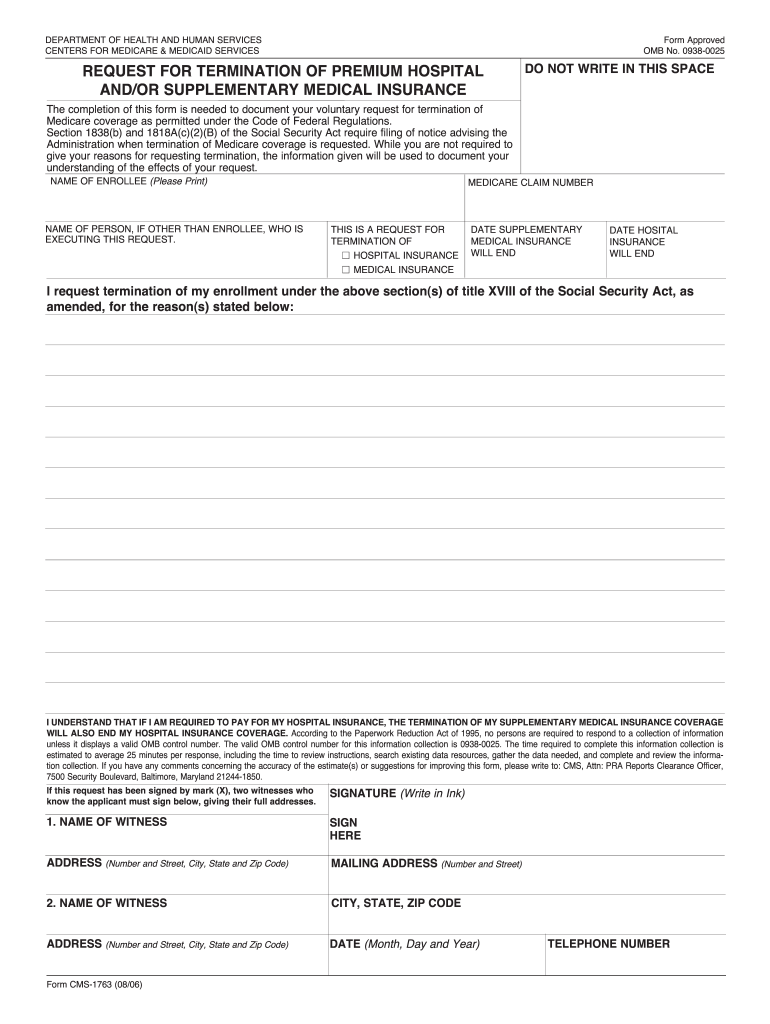



Who needs a Form CMS-1763?
A person who wants to terminate their Medicare coverage (Part B section) should file CMS-1763 to confirm their voluntary decision.
What is Form CMS-1763 for?
While an applicant is not required to give their reasons for requesting termination, the information given by this form will be used as an attestation of understanding the consequences of such refusal. If an applicant is required to pay for their hospital insurance, the termination of their supplementary medical insurance coverage will also end their hospital insurance coverage. Also, an applicant might have to pay a late penalty if they want to re-enroll in the program in the future.
Is Form CMS-1763 accompanied by other forms?
This form does not require the support of other documents and can be filed as it is.
When is Form CMS-1763 due?
You can submit this form at any time, whenever it becomes necessary.
How do I fill out Form CMS-1763?
You must complete this form during an interview with a Social Security representative; you can do this either during a personal interview at a Social Security office or on the phone. Either way, you will have to enlist the testimony of two witnesses who must assure the finished form before submission.
Where do I send Form CMS-1763?
Signed and completed form must be sent to the nearest Social Security office.