Last updated on Apr 12, 2026

Get the free Member Data Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is member data change form
The Member Data Change Form is a healthcare document used by Peach State members to update personal information and request a change of Primary Care Physician (PCP).
pdfFiller scores top ratings on review platforms
Who needs member data change form?
Explore how professionals across industries use pdfFiller.

Member data change form is needed by:
-
Peach State Health Plan members.
-
Responsible parties for members.
-
Healthcare providers coordinating member care.
-
Medicaid recipients in Georgia.
-
Individuals needing to change their Primary Care Physician.
-
Patient advocates assisting with healthcare processes.
Comprehensive Guide to member data change form
What is the Member Data Change Form?
The Member Data Change Form is a crucial document designed for members of Peach State to update their personal information systematically. By utilizing this form, members can ensure that their healthcare providers have the most current details, which is vital for effective medical care.
This healthcare form is necessary whenever a member experiences life changes, such as relocating or altering their healthcare provider. Members can make various changes, including updating their address, contact information, and Primary Care Physician (PCP) details.
Purpose and Benefits of the Member Data Change Form
Accurate and updated member information is essential for healthcare delivery. Using the Member Data Change Form not only streamlines the process of reporting changes but also ensures that healthcare providers can offer timely and relevant services.
-
The form facilitates smooth changes to Primary Care Physician details, making transitions seamless.
-
Accurate information reduces errors in communication between members and healthcare providers.
Who Needs the Member Data Change Form?
The form is intended for members of Peach State and their responsible parties who are eligible to submit updates. Multiple scenarios necessitate the use of this form, such as moving to a new address or changing to a different Primary Care Physician.
It's important to note that the legal responsibility for signing the form typically falls on the member or a designated responsible party.
How to Fill Out the Member Data Change Form Online
Accessing the Member Data Change Form online involves a straightforward process. Members should start by entering their personal information, including their name and Medicaid ID, followed by the relevant PCP information.
-
Utilize pdfFiller’s editing features to digitalize the form filling process.
-
Make sure to provide specific details for any requested changes, especially regarding the reason for a new PCP.
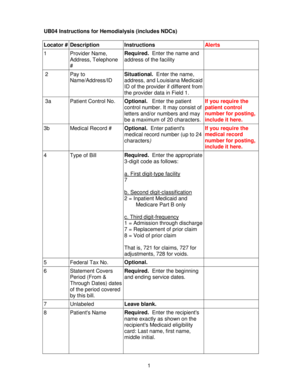
Field-by-Field Instructions for the Member Data Change Form
Filling out the Member Data Change Form requires careful attention to detail. Essential fields include the member's name, Medicaid ID, current address, and up-to-date contact information.
-
When entering PCP details, ensure accuracy to avoid discrepancies.
-
Clearly state your reasons for requesting a change, which can expedite processing.
Review and Validation Checklist
Before submitting the Member Data Change Form, users should double-check essential items. Validating the signature and ensuring all information is accurate is crucial for a successful submission.
-
Verify that all contact details are correct for any necessary follow-ups.
-
Ensure that the form is complete to prevent delays in processing.
Submission Methods and Delivery Options for the Member Data Change Form
Once the form is completed, multiple submission methods are available for members to choose from. Options include faxing or emailing the form directly to the Member Services Department.
Members should also be aware of the expected processing time once the form is submitted, which can vary based on volume and complexity of the changes requested.
Security and Compliance for the Member Data Change Form
Submitting the Member Data Change Form involves sensitive information, making data security a top priority. pdfFiller implements robust security measures, including 256-bit encryption, to protect personal data during the filling and submission process.
Additionally, adherence to HIPAA compliance underscores the importance of safeguarding member information throughout this process.
Benefits of Using pdfFiller for Completing the Member Data Change Form
Leveraging pdfFiller enhances the experience of filling out the Member Data Change Form. The platform offers key features such as easy editing, electronic signing, and the convenience of cloud storage.
Using this digital platform not only simplifies the form-filling and submission process but also provides users with an efficient and secure environment.
Start Filling Out Your Member Data Change Form Today!
Engage with pdfFiller today to streamline the process of updating your member information. Enjoy the ease of filling out the Member Data Change Form online with enhanced security and support.
How to fill out the member data change form
-
1.Access the Member Data Change Form on pdfFiller by searching for the form name. Look for the document in the healthcare forms section.
-
2.Open the form and familiarize yourself with its layout. Identify the fillable fields and checkboxes provided for your responses.
-
3.Gather all necessary information before you start filling out the form. This includes your personal details such as name, Medicaid ID, address, and contact information.
-
4.Complete the required fields including your information and the details of the new Primary Care Physician you wish to request.
-
5.Provide the reason for changing your PCP in the designated section of the form.
-
6.Review all your entries carefully to ensure accuracy. Look for any missed fields or spelling errors in your contact information and PCP details.
-
7.Finalize the form by signing in the appropriate section, either by using an electronic signature or by printing and signing it physically.
-
8.Once completed, save your form within pdfFiller for your records. Use the download option if you need to keep a copy.
-
9.Submit the form by faxing it to the Member Services Department as specified in the instructions. Ensure you have the correct fax number.

Who is eligible to use the Member Data Change Form?
The form is intended for members of the Peach State Health Plan and their responsible parties who need to update contact information or change their Primary Care Physician.
Is there a deadline for submitting this form?
While specific deadlines may vary, it’s recommended to submit the form as soon as changes occur to ensure accurate and updated records with your healthcare provider.
How do I submit the Member Data Change Form?
The form must be faxed to the Member Services Department after signing. Ensure you have included all necessary information before sending.
What supporting documents are required with the form?
No additional supporting documents are typically required; however, having your Medicaid ID and any relevant identification ready is helpful for filling out the form.
What are common mistakes to avoid when filling out this form?
Ensure all fields are completed accurately, particularly your contact information and PCP details. Slipping errors or missing signatures may delay processing.
How long does it take for my changes to be processed?
Processing times can vary, but it usually takes a few business days for updates to reflect in your healthcare records after submission.
Can I make changes to the form after submission?
Once submitted, you will need to submit a new Member Data Change Form to make any additional changes. Be sure to review it thoroughly before sending again.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.