Add or replace text, adjust formatting, insert legally binding eSignatures, and send documents for signing without hopping between apps.
WCIF Health Care Provider Biometric Screening Form 2013-2025 free printable template
Show details
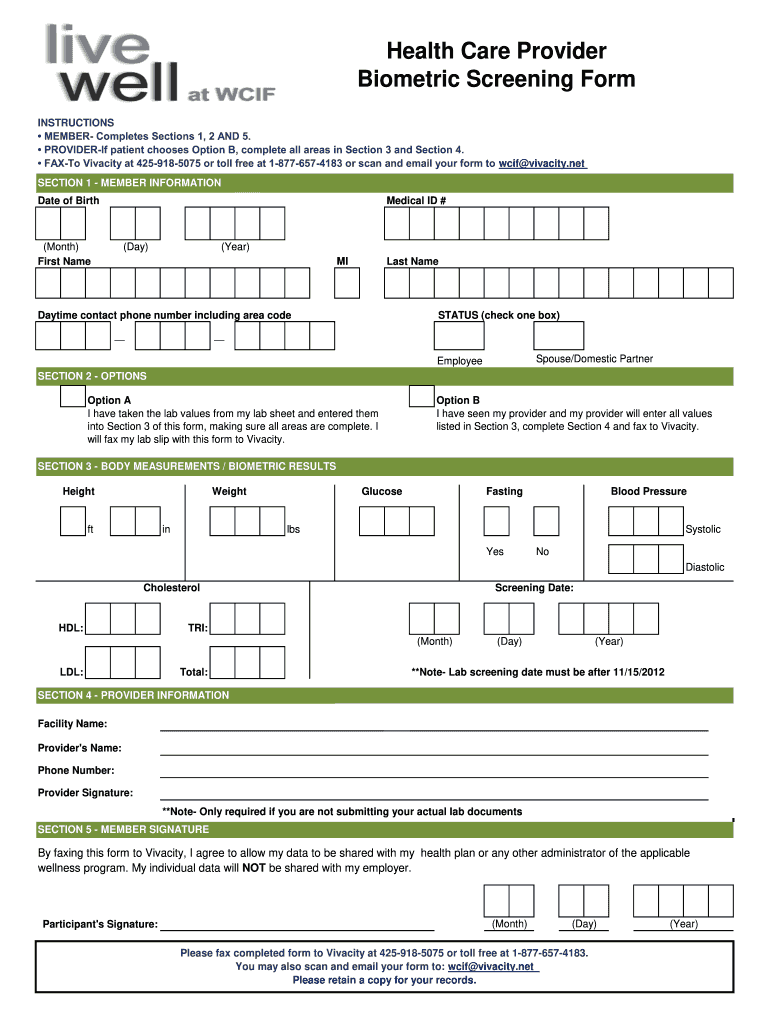
Health Care Provider Biometric Screening Form INSTRUCTIONS MEMBER- Completes Sections 1 2 AND 5. PROVIDER-If patient chooses Option B complete all areas in Section 3 and Section 4. SECTION 3 - BODY MEASUREMENTS / BIOMETRIC RESULTS Height ft in Glucose Fasting Blood Pressure lbs Systolic Yes No Diastolic Cholesterol HDL Screening Date TRI LDL Total Note- Lab screening date must be after 11/15/2012 SECTION 4 - PROVIDER INFORMATION Facility Name Provider s Name Phone Number Provider Signature...Note- Only required if you are not submitting your actual lab documents By faxing this form to Vivacity I agree to allow my data to be shared with my health plan or any other administrator of the applicable wellness program. My individual data will NOT be shared with my employer. FAX-To Vivacity at 425-918-5075 or toll free at 1-877-657-4183 or scan and email your form to wcif vivacity. net SECTION 1 - MEMBER INFORMATION Date of Birth Month First Name Medical ID Day Year MI Last Name Daytime...contact phone number including area code STATUS check one box Spouse/Domestic Partner Employee SECTION 2 - OPTIONS Option A I have taken the lab values from my lab sheet and entered them into Section 3 of this form making sure all areas are complete. I will fax my lab slip with this form to Vivacity. I have seen my provider and my provider will enter all values listed in Section 3 complete Section 4 and fax to Vivacity. Participant s Signature Please fax completed form to Vivacity at...425-918-5075 or toll free at 1-877-657-4183. FAX-To Vivacity at 425-918-5075 or toll free at 1-877-657-4183 or scan and email your form to wcif vivacity. net SECTION 1 - MEMBER INFORMATION Date of Birth Month First Name Medical ID Day Year MI Last Name Daytime contact phone number including area code STATUS check one box Spouse/Domestic Partner Employee SECTION 2 - OPTIONS Option A I have taken the lab values from my lab sheet and entered them into Section 3 of this form making sure all areas...are complete. net SECTION 1 - MEMBER INFORMATION Date of Birth Month First Name Medical ID Day Year MI Last Name Daytime contact phone number including area code STATUS check one box Spouse/Domestic Partner Employee SECTION 2 - OPTIONS Option A I have taken the lab values from my lab sheet and entered them into Section 3 of this form making sure all areas are complete. I will fax my lab slip with this form to Vivacity. I have seen my provider and my provider will enter all values listed in...Section 3 complete Section 4 and fax to Vivacity. FAX-To Vivacity at 425-918-5075 or toll free at 1-877-657-4183 or scan and email your form to wcif vivacity. net SECTION 1 - MEMBER INFORMATION Date of Birth Month First Name Medical ID Day Year MI Last Name Daytime contact phone number including area code STATUS check one box Spouse/Domestic Partner Employee SECTION 2 - OPTIONS Option A I have taken the lab values from my lab sheet and entered them into Section 3 of this form making sure all...areas are complete. I will fax my lab slip with this form to Vivacity. I have seen my provider and my provider will enter all values listed in Section 3 complete Section 4 and fax to Vivacity.
pdfFiller is not affiliated with any government organization
Fill out, sign, and share forms from a single PDF platform
Manage all your documents quickly and securely in the cloud.
Edit and sign in one place
Create professional forms
Add and customize fillable fields to tailor each form to your needs and ensure easy completion without printing and scanning.
Simplify data collection
Quickly share forms via email or a secure link, enabling anyone to complete forms online in seconds, on any device.
Manage forms centrally
Keep all your forms and templates organized in one secure, cloud-based platform, track changes easily, and export documents in any format.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
Understanding the WCIF Health Care Provider Form
What is the WCIF Health Care Provider Form
The WCIF Health Care Provider Form is a document designed for individuals participating in health and wellness programs. It enables members to submit their biometric screening information to their health plans. This form plays a crucial role in ensuring that health data is accurately collected and shared while maintaining participant confidentiality. By filling out this form, members take a proactive step in managing their health care needs.
When to Use the WCIF Health Care Provider Form
This form should be used when a member seeks to report results from a biometric screening, either conducted by a medical provider or through self-reporting. Members are encouraged to use this form when applying for wellness incentives or health plan benefits related to health screenings, as well as to improve their overall health management.
How to Fill the WCIF Health Care Provider Form
Filling out the WCIF Health Care Provider Form involves several key steps: First, the member must complete Sections One, Two, and Five, providing personal and contact information. Depending on the option chosen, the provider may need to complete Sections Three and Four. It is essential to ensure all fields are filled accurately and completely, especially the required measurements and provider information, to avoid delays in processing.
Required Documents and Information
To successfully submit the WCIF Health Care Provider Form, members need to provide essential information including their date of birth, medical ID number, and contact details. Additionally, if choosing Option B, a current lab report must accompany the form. Accurate measurements like height, weight, blood pressure, and cholesterol levels are also necessary to fulfill the form's requirements.
Benefits of Using the WCIF Health Care Provider Form
Using the WCIF Health Care Provider Form offers several benefits to members. It streamlines the process of submitting critical health data to health plans, facilitates access to wellness incentives, and supports better personal health management. Moreover, it ensures that individual health information is handled securely while maintaining privacy.
Common Errors and Troubleshooting
Several common errors might occur when filling out the WCIF Health Care Provider Form. These include incomplete sections, incorrect height and weight entries, or failure to include necessary documentation such as lab results. Members should review the form carefully before submission, ensuring all required fields are filled and accurate. If issues arise, contacting customer support for clarification on specific sections can help resolve any uncertainties.
Review and Validation Checklist
Before submitting the WCIF Health Care Provider Form, members are advised to use a review checklist that includes verifying personal information, ensuring all measurements are accurately recorded, and confirming that any accompanying documents are included. Additionally, reviewing the signature section is critical to ensure authorization is provided. This checklist can prevent common submission errors and facilitate a smoother process.
Frequently Asked Questions about biometric screening form pdf
What is the purpose of the WCIF Health Care Provider Form?
The form is designed to collect biometric screening data from members, allowing them to share important health information with their health plans and qualify for wellness programs.
Who needs to complete the WCIF Health Care Provider Form?
Members participating in wellness programs and seeking to report their biometric screening results need to complete this form.
pdfFiller scores top ratings on review platforms
SO FAR SO GOOD A LIFE SAFER
it was quick .....
na
ok
So far I've had a good experience
SO FAR ITS GOOD.
Related pages
Related to WCIF Health Care Provider Biometric Screening






Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.