Last updated on May 28, 2014

Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient medical history form
The Patient Medical History Form is a medical document used by healthcare providers to collect detailed medical history information from patients.
pdfFiller scores top ratings on review platforms
Who needs patient medical history form?
Explore how professionals across industries use pdfFiller.

Patient medical history form is needed by:
-
Healthcare providers seeking patient medical details
-
Patients registering for medical services
-
Administrators managing patient intake forms
-
Insurance representatives processing claims
-
Medical researchers analyzing patient data
-
Assistants aiding in patient documentation
Comprehensive Guide to patient medical history form
What is the Patient Medical History Form?
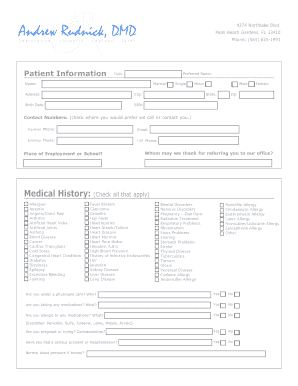
The Patient Medical History Form is a crucial document used in healthcare settings to gather comprehensive medical history from patients. Its main purpose is to collect vital information that aids healthcare providers in understanding a patient's health background. Typically, the form includes sections covering various health conditions, medications taken, and family history. Additionally, it is important to note that the form requires the patient's signature to confirm information accuracy and consent for treatment.
Purpose and Benefits of the Patient Medical History Form
This form serves multiple purposes that enhance care quality for both patients and providers. By ensuring comprehensive collection of a patient’s medical background, the form allows healthcare providers to make informed decisions regarding treatment. Furthermore, it streamlines the patient registration and intake process, saving time and reducing the likelihood of errors. Ultimately, the patient medical history form is essential for effective healthcare delivery.
Key Features of the Patient Medical History Form
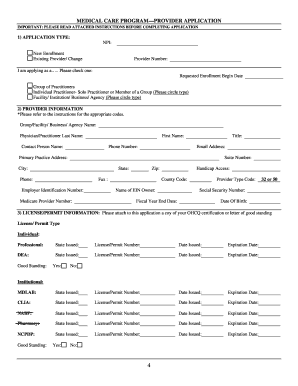
The Patient Medical History Form boasts several key features that facilitate thorough data collection. It contains fillable sections for documenting health conditions, medications, and family history. To accommodate diverse patient needs, the form includes checkboxes and blank fields. Additionally, it ensures that the patient agrees to payment terms and any insurance claims, reinforcing the importance of consent in healthcare transactions.
Who Needs the Patient Medical History Form?
The Patient Medical History Form is designed for a wide range of users. Primarily, patients visiting a new healthcare provider will need to complete this form to provide crucial health insights. Moreover, individuals requiring specialized treatments or assessments, particularly in eye care, will benefit from submitting their medical history through this form. It is applicable in both clinical environments and telehealth settings, ensuring accessibility for all patients.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
Filling out the Patient Medical History Form online is a straightforward process. Follow these step-by-step instructions to ensure accuracy:
-
Begin by entering your personal information, including name, date of birth, and contact details.
-
Complete the sections related to your previous medical conditions, ensuring to specify all relevant diagnoses.
-
List current medications, including dosages and frequencies.
-
Provide information on family medical history, detailing any hereditary conditions.
-
Review all entries for completeness and accuracy before submission.
Taking these steps helps ensure that your healthcare provider has the most accurate and complete information for effective treatment planning.
Common Errors and How to Avoid Them
When completing the Patient Medical History Form, various common errors can occur. Frequent mistakes include missing important information or entering incorrect medication dosages. To avoid these pitfalls, consider implementing the following strategies:
-
Double-check all entries to ensure no fields are left blank.
-
Verify medication names and dosages against your current prescriptions.
-
Ensure clarity in handwriting, particularly for non-digital formats.
By being mindful of these errors, you can improve the accuracy of your submitted form.
How to Sign the Patient Medical History Form
Signing the Patient Medical History Form is an essential step, as it confirms consent and authorizes healthcare providers to engage in treatment. There are two primary signing methods available: digital signatures and traditional signatures. For those opting for eSigning, pdfFiller provides an intuitive interface for completing this process. Remember, your signature validates the information provided and is necessary for insurance claims.
Where to Submit the Patient Medical History Form
Once completed, the Patient Medical History Form needs to be submitted appropriately. Users have several options for submission:
-
Submit electronically through a secure online portal for quick processing.
-
Opt for physical submission by mailing or hand-delivering the form to the healthcare provider.
Be sure to inquire about tracking submission status and be aware of any associated fees or processing times to avoid delays in care.
Security and Compliance for the Patient Medical History Form
Protecting sensitive patient information is critical when handling the Patient Medical History Form. pdfFiller employs robust security measures, including 256-bit encryption and compliance with HIPAA regulations. Patients should also be aware of their privacy rights when filling out the form, ensuring their information remains secure while utilizing online platforms.
Utilizing pdfFiller for Your Patient Medical History Form Needs
Leveraging pdfFiller's cloud-based platform can significantly enhance your experience with the Patient Medical History Form. This platform allows for easy editing, eSigning, and secure sharing of completed forms with healthcare providers. Moreover, users can access their forms anytime, reinforcing the convenience and security of managing sensitive documents online.
How to fill out the patient medical history form
-
1.Access pdfFiller and log in to your account or create a free account if you are not registered.
-
2.Navigate to the search bar and enter 'Patient Medical History Form' to locate the form quickly.
-
3.Click on the form from the search results to open it in the pdfFiller interface.
-
4.Review the form specifications and ensure you have all necessary medical information handy, including medications, health conditions, and family health history.
-
5.Use the toolbar to fill in the required fields. Click on checkboxes for applicable health issues and type in your medications where indicated.
-
6.Make sure to complete all sections by providing accurate and thorough information about your medical history.
-
7.After filling in all necessary fields, review the information for accuracy. Correct any mistakes before finalizing.
-
8.Once reviewed, save the form by clicking the 'Save' button. You can also download it for your records or print it directly.
-
9.If submitting electronically, select the 'Submit' option to send the completed form to your healthcare provider directly through pdfFiller.

Who needs to fill out the Patient Medical History Form?
Any patient visiting a healthcare provider, such as a doctor or a specialist, is required to complete the Patient Medical History Form. This helps providers understand the patient's overall health profile and medical background.
What information is typically required on this form?
The Patient Medical History Form generally requires information about existing health conditions, medications currently being taken, family medical history, and lifestyle factors. Gather detailed information before starting the form.
How can I submit the completed form?
You can submit the completed Patient Medical History Form through pdfFiller by selecting the 'Submit' option. Ensure you follow any specific submission procedures outlined by your healthcare provider.
Are there any deadlines for submitting this form?
While there are typically no strict deadlines for filling out the Patient Medical History Form, it's recommended to complete it before your scheduled appointment to ensure the healthcare provider has adequate time to review your information.
What common mistakes should I avoid when filling out the form?
Common mistakes include leaving sections blank, providing inaccurate medication details, or neglecting to sign the form. Double-check all entries to avoid delays in processing your information.
How quickly can I expect my information to be processed?
Processing times for the Patient Medical History Form can vary by provider. Generally, information is reviewed on the same day, but follow up with your healthcare provider for specific time frames.
Is notarization required for this form?
No, notarization is not required for the Patient Medical History Form. It only requires the patient's signature to confirm the information provided and authorize insurance claims.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.