Get the free Dental Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
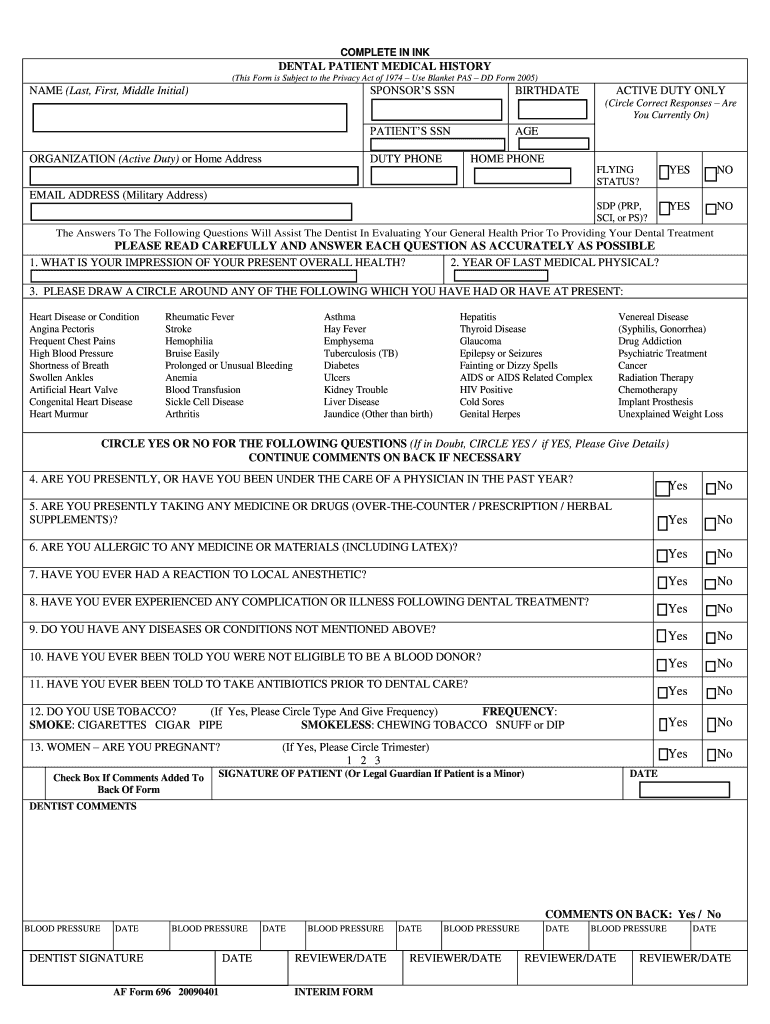
What is dental patient medical history
The Dental Patient Medical History Form is a medical document used by dental clinics to collect essential health information from patients prior to treatment.
pdfFiller scores top ratings on review platforms
Who needs dental patient medical history?
Explore how professionals across industries use pdfFiller.

Dental patient medical history is needed by:
-
Patients seeking dental treatment
-
Dentists requiring patient medical history
-
Dental clinics managing patient intake
-
Healthcare providers ensuring patient safety
-
Insurance companies needing medical documentation
How to fill out the dental patient medical history
-
1.Access the Dental Patient Medical History Form on pdfFiller by searching for the form name in the search bar or navigating to the healthcare forms section.
-
2.Open the form and familiarize yourself with the layout, which includes a series of fillable fields and checkboxes designed for your responses.
-
3.Before starting, gather necessary information such as personal details, medical history, current medications, allergies, and any specific health conditions that apply to you.
-
4.Navigate through the document by clicking into the fields; you can type directly into text boxes or select options from dropdown menus or checkboxes as applicable.
-
5.Fill in each required section accurately, ensuring that all information provided is current and truthful, as it will assist your dentist in providing appropriate care.
-
6.Once all fields are completed, review your entries carefully, making sure there are no errors or omitted information; double-check particularly for any specified conditions or allergies.
-
7.Finalize the form by signing digitally in the designated area to confirm the accuracy of your provided information and your consent for treatment.
-
8.Lastly, save your completed form on pdfFiller. You can download it as a PDF for your records or select the submit option to send it directly to your dentist or clinic.

Who needs to complete the Dental Patient Medical History Form?
Patients who are about to receive dental treatment must complete the Dental Patient Medical History Form to provide their dentist with crucial health information necessary for safe care.
How do I submit the completed form?
After filling out the form on pdfFiller, you can submit it directly through the platform or download it to print and bring to your dental appointment.
Are there specific deadlines for submitting this form?
While there are no strict deadlines, it is advisable to complete the Dental Patient Medical History Form at least a few days before your dental appointment to ensure sufficient time for your dentist to review it.
What should I do if I make a mistake while filling out the form?
If you make an error on the form, simply navigate back to the respective field in pdfFiller and correct your information before finalizing and submitting the document.
What information is typically required on this form?
You will need to provide personal details such as your name and contact information, as well as your medical history, current medications, known allergies, and any chronic health conditions.
Is the Dental Patient Medical History Form confidential?
Yes, the information you provide on the Dental Patient Medical History Form is confidential and is only shared with your dentist or necessary healthcare personnel involved in your care.
Can I fill out the form on my mobile device?
Yes, pdfFiller allows you to fill out the Dental Patient Medical History Form on mobile devices, making it convenient to complete it anytime and anywhere.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.