Last updated on Oct 29, 2014
Get the free Health Net Open Enrollment Medical Plan Change Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
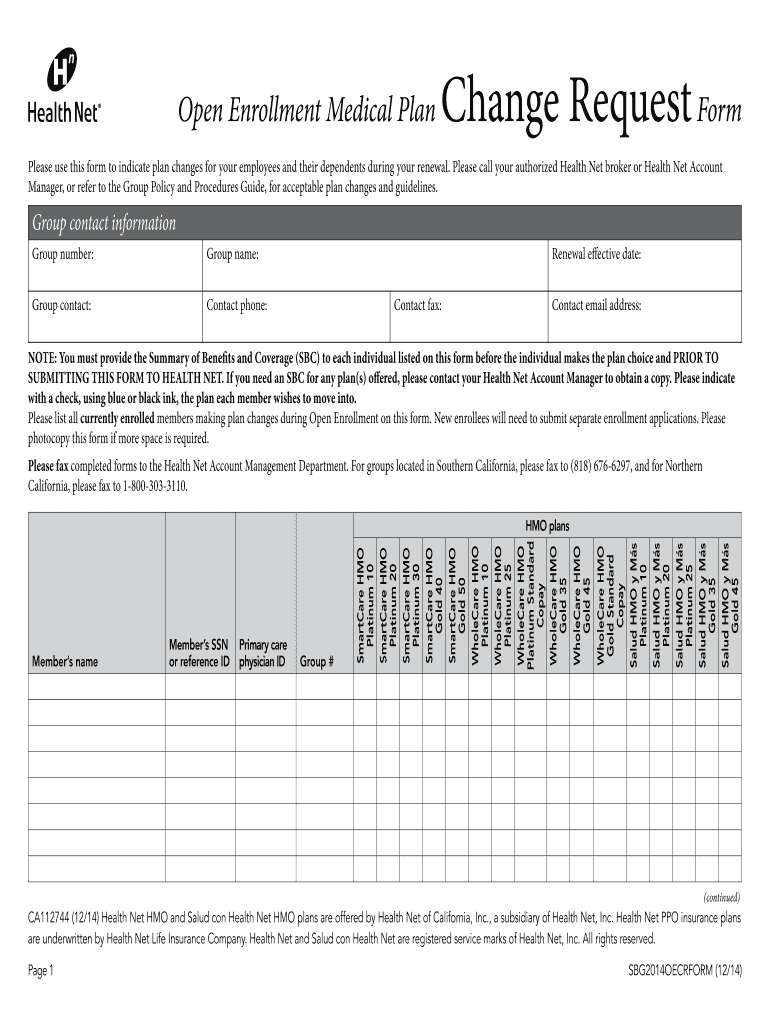
What is Health Net Plan Change Form
The Health Net Open Enrollment Medical Plan Change Request Form is a medical consent document used by employers in California to request plan changes for their employees and dependents during the renewal period.
pdfFiller scores top ratings on review platforms
Who needs Health Net Plan Change Form?
Explore how professionals across industries use pdfFiller.

Health Net Plan Change Form is needed by:
-
Employers in California managing employee health plans
-
Group contacts responsible for plan selection
-
Authorized representatives assisting with medical plan changes
-
Employees looking to update their medical plan information
-
Dependents of employees affected by plan changes
-
Human resources professionals overseeing employee benefits
Comprehensive Guide to Health Net Plan Change Form
What is the Health Net Open Enrollment Medical Plan Change Request Form?
The Health Net Open Enrollment Medical Plan Change Request Form is a vital document used by employers in California during the open enrollment period. This form enables employees to request changes to their medical coverage. Users of the form can include group contacts and authorized representatives, allowing for various adjustments related to health care plans.
Specifically, this form facilitates changes such as switching from one plan to another, modifying coverage levels, and updating dependent information.
Purpose and Benefits of the Health Net Open Enrollment Medical Plan Change Request Form
This form serves a clear purpose for both employers and employees, providing a structured means to request adjustments in their medical insurance coverage. By using the Health Net Open Enrollment form, employees can better manage their health plans and ensure that their dependents receive appropriate coverage.
Key benefits include:
-
Streamlined process for revising health care coverage.
-
Opportunities for employees to select plans that best fit their needs.
-
Improved understanding of available medical coverage options.
Key Features of the Health Net Open Enrollment Medical Plan Change Request Form
The Health Net Open Enrollment Medical Plan Change Request Form contains several essential components, including member details and plan selection checkboxes. Users must complete fields such as 'Group number:', 'Member’s name:', and 'Member’s SSN' to ensure accurate processing.
Additionally, each submission requires a Summary of Benefits and Coverage (SBC) document that outlines the specific benefits associated with the chosen plan. This is crucial for facilitating informed decisions regarding healthcare options.
Who Needs the Health Net Open Enrollment Medical Plan Change Request Form?
Primary users of this form include employers and authorized representatives within organizations. These individuals play a significant role in guiding employees through the open enrollment process.
Scenarios in which the form is necessary include:
-
When an employee needs to change their current health plan.
-
When adding or removing dependents from coverage.
-
During annual open enrollment periods for group medical plans.
How to Fill Out the Health Net Open Enrollment Medical Plan Change Request Form Online: Step-by-Step
Filling out the Health Net form online is a straightforward process when using pdfFiller. Follow these steps to ensure a smooth completion:
-
Access the form on pdfFiller and select the appropriate template.
-
Enter the 'Group number:' for identification purposes.
-
Fill in the 'Member’s name:' and 'Member’s SSN' accurately.
-
Choose the desired health plan options using the checkboxes provided.
-
Review all entries for accuracy before submission.
Common Errors and How to Avoid Them When Submitting the Health Net Open Enrollment Medical Plan Change Request Form
When completing the form, it's vital to avoid common mistakes that can lead to processing delays. Frequent errors include:
-
Omitting required information such as member details.
-
Failing to select the appropriate plan checkboxes.
-
Submitting the form without the necessary Summary of Benefits and Coverage (SBC).
To ensure accuracy and completeness, double-check entries and confirm that all sections of the form are filled out before submission.
Submission Methods and Delivery for the Health Net Open Enrollment Medical Plan Change Request Form
The Health Net Open Enrollment Medical Plan Change Request Form can be submitted through various methods, including online and traditional mail options. After completing the form, users should confirm submission through the chosen method to ensure it reaches Health Net.
Post-submission, it is advisable to track the status and ensure confirmation from Health Net for peace of mind.
Security and Compliance for the Health Net Open Enrollment Medical Plan Change Request Form
Data protection and compliance are crucial when handling the Health Net Open Enrollment Medical Plan Change Request Form. Strict HIPAA compliance measures must be followed to safeguard personal and sensitive information.
Employers should prioritize secure document handling to maintain privacy and protect employee data throughout the enrollment process.
How pdfFiller Can Simplify Your Health Net Open Enrollment Medical Plan Change Request Form Experience
pdfFiller enhances the experience of filling out the Health Net Open Enrollment Medical Plan Change Request Form with its user-friendly interface. Key features include easy document editing, eSigning capabilities, and secure cloud storage.
By using pdfFiller, users benefit from streamlined workflows, improved security for sensitive documents, and convenient access to forms from any device.
Additional Resources and Support for the Health Net Open Enrollment Medical Plan Change Request Form
For further information regarding the Health Net Open Enrollment Medical Plan Change Request Form, users can find additional resources and assistance through official channels. It is advisable to look for:
-
Links to related forms and guidelines relevant to the California medical plan changes.
-
Customer support services for personalized assistance.
How to fill out the Health Net Plan Change Form
-
1.To begin, access the Health Net Open Enrollment Medical Plan Change Request Form on pdfFiller by searching for the form title in the search bar.
-
2.Once you've located the form, click on it to open and display the editable PDF interface.
-
3.Before you start filling out the form, gather the necessary information, including group contact details, member’s name, Social Security Number, and the desired plan selections.
-
4.Navigate through the form and click on each blank field to enter the relevant information directly in the provided spaces.
-
5.Use checkboxes for selecting the applicable medical plans and ensure that all necessary fields are filled out completely for validity.
-
6.Review the completed form carefully, checking for any missing information and confirming that all entries are accurate.
-
7.Once satisfied with the information provided, use pdfFiller's options to save your completed form.
-
8.You can download the form directly to your device or submit it electronically to Health Net according to your preference.

Who is eligible to use the Health Net Open Enrollment Medical Plan Change Request Form?
Employers in California who provide health insurance to their employees can use this form to request changes during the open enrollment period.
What documents are required when submitting this form?
You must accompany the form with a Summary of Benefits and Coverage (SBC) for each individual covered under the medical plan.
What is the deadline for submitting the form?
The form must be submitted during the designated open enrollment period. Check the specific dates provided by Health Net each year.
How do I submit the Health Net Open Enrollment Medical Plan Change Request Form?
You can submit the completed form electronically through pdfFiller or print and send it via mail to Health Net, following their submission guidelines.
What information do I need to complete the form accurately?
You need group identification details, member information including names and SSNs, as well as selections of medical plans that you intend to change to.
What are common mistakes to avoid while filling out this form?
Ensure that all required fields are filled out completely, double-check member information for accuracy, and make sure to attach the necessary SBCs.
What is the processing time for changes made through this form?
Processing times can vary, but typically, changes are confirmed shortly after submission depending on Health Net's workflow and requirements.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.