Last updated on May 5, 2026
Canada St. Josephs Care Group CF-0327 2016-2026 free printable template
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Canada St. Josephs Care Group CF-0327
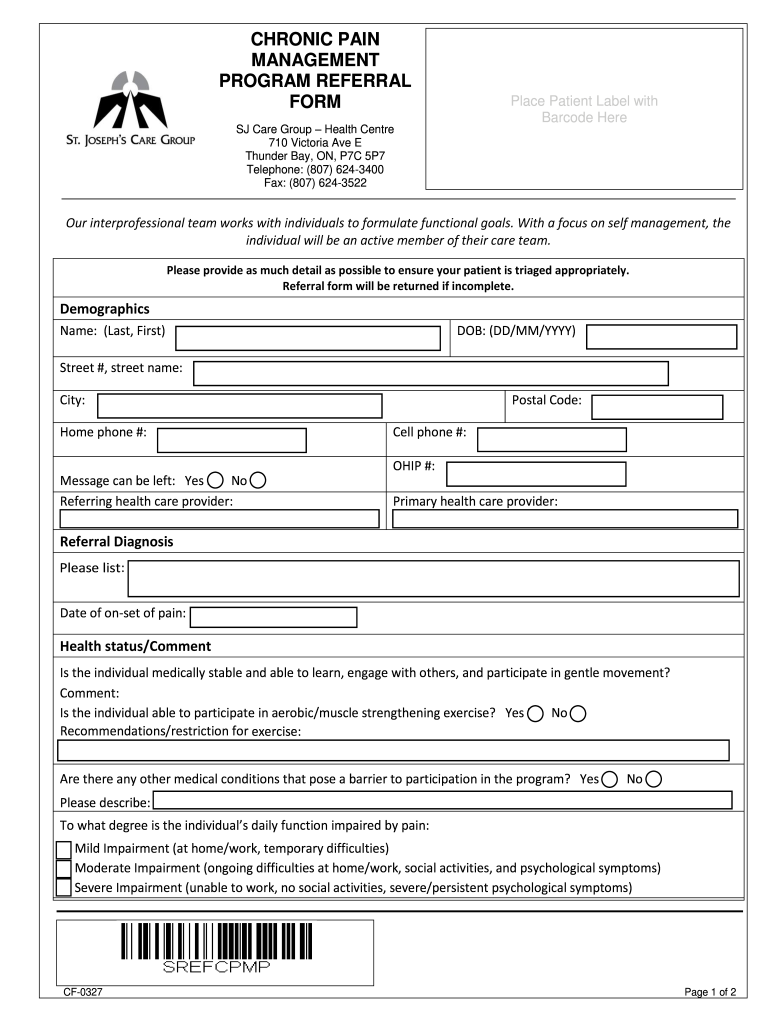
The Chronic Pain Management Program Referral Form is a healthcare document used by providers in Ontario, Canada, to refer patients for chronic pain management services.
pdfFiller scores top ratings on review platforms
Who needs Canada St. Josephs Care Group CF-0327?
Explore how professionals across industries use pdfFiller.

Canada St. Josephs Care Group CF-0327 is needed by:
-
Healthcare providers seeking to refer patients with chronic pain.
-
Clinics specializing in pain management and rehabilitation services.
-
Patients needing access to chronic pain management programs.
-
Medical administrators handling patient intake and referrals.
-
Insurance companies assessing patient treatments and programs.
Comprehensive Guide to Canada St. Josephs Care Group CF-0327
What is the Chronic Pain Management Program Referral Form?
The Chronic Pain Management Program Referral Form is a critical document used by healthcare providers in Ontario, Canada, to facilitate the referral of patients to specialized chronic pain management services. This form is instrumental in gathering essential patient information, including demographics, health status, and the specific interventions requested. Healthcare providers benefit from this organized approach, which enhances the overall referral process.
By utilizing the chronic pain management referral form, practitioners can ensure that they meet the healthcare needs of their patients effectively, streamlining their ability to access specialized care.
Purpose and Benefits of the Chronic Pain Management Program Referral Form
The primary purpose of this form is to provide a structured means for patients to gain access to specialized chronic pain management care. This facilitates a clear pathway for healthcare providers, enabling a more efficient response to patient needs. The form allows for improved communication between referring practitioners and specialists, which is vital for effective patient care.
Additionally, the form empowers patients by enhancing their engagement in managing chronic pain, which can lead to better health outcomes. Healthcare providers also benefit from streamlined processes, allowing them to focus more on patient care rather than administrative tasks.
Key Features of the Chronic Pain Management Program Referral Form
The Chronic Pain Management Program Referral Form includes several critical sections that play a vital role in the referral process:
-
Demographic information of the patient
-
Referral diagnosis and reasons for referral
-
Details regarding health status
-
Signatory requirements to validate the referral
-
Sections for additional comments and triage needs
Each of these features ensures that all necessary information is accurately captured, thus aiding in effective patient care.
Who Needs the Chronic Pain Management Program Referral Form?
The referral form is essential for various stakeholders, including healthcare providers and patients. It is particularly relevant to specific demographics suffering from different types of chronic pain, such as fibromyalgia or arthritis. Various healthcare professionals, from general practitioners to specialists, play a significant role in utilizing this form to improve patient management.
Understanding the specific needs of patients and the intricacies of the referral process is essential for effective chronic pain treatment.
Eligibility Criteria for the Chronic Pain Management Program Referral Form
To qualify for the Chronic Pain Management Program, patients must meet certain eligibility criteria:
-
Diagnosis of specific chronic pain conditions
-
Evidence of prior treatment and management efforts
-
Residency requirements in Ontario
These criteria ensure that only those who truly need specialized care can access the program, thereby optimizing the use of healthcare resources.
How to Fill Out the Chronic Pain Management Program Referral Form Online (Step-by-Step)
Filling out the Chronic Pain Management Program Referral Form online is straightforward. Here’s a step-by-step guide:
-
Access the Chronic Pain Management Program Referral Form on a secure platform.
-
Gather all necessary information, including patient demographics and medical history.
-
Carefully fill out each field to ensure accuracy and clarity.
-
Review the completed form for any mistakes or missing information.
-
Submit the form electronically, ensuring all required signatures are obtained.
By following these steps, healthcare providers can avoid common mistakes and ensure a smooth referral process.
Common Errors and How to Avoid Them
When filling out the Chronic Pain Management Program Referral Form, there are several frequent mistakes to be mindful of:
-
Omitting demographic details or signatures
-
Providing unclear or ambiguous information in the referral diagnosis
-
Neglecting to include all necessary supporting documents
Double-checking these elements before submission can significantly reduce errors and expedite the referral process for patients.
How to Submit the Chronic Pain Management Program Referral Form
Submitting the Chronic Pain Management Program Referral Form can be done through multiple methods:
-
Online submission via a secure platform
-
Mailing the completed form to the appropriate healthcare facility
-
Delivering the form in person to the specified location
Ensure that all required supporting materials accompany your submission and adhere to any specified deadlines for processing.
Security and Compliance for the Chronic Pain Management Program Referral Form
Handling sensitive patient information requires stringent security measures. The Chronic Pain Management Program Referral Form adheres to essential compliance standards, including HIPAA and GDPR, ensuring patient privacy. Encryption measures are in place to guarantee the safety of document management and sharing processes, providing peace of mind to both healthcare providers and patients.
Maximize Your Efficiency with pdfFiller
Healthcare providers can enhance their form-filling experience by utilizing pdfFiller. This robust platform simplifies editing, eSigning, and sharing the Chronic Pain Management Program Referral Form, making the process more efficient. With its user-friendly features, healthcare providers can focus on delivering quality patient care while managing forms securely in a cloud-based environment.
How to fill out the Canada St. Josephs Care Group CF-0327
-
1.To access the Chronic Pain Management Program Referral Form on pdfFiller, visit the platform and search for the form by name in the search bar.
-
2.Once located, click on the form to open it in the editor interface. Familiarize yourself with the layout and sections to ensure a smooth filling process.
-
3.Before filling out the form, gather all necessary patient information such as demographics, medical history, referral diagnosis, and any specific interventions required for better accuracy.
-
4.Begin by entering the patient's details in the designated fields including their full name, date of birth, and contact information.
-
5.Next, provide detailed information regarding the referral diagnosis, including relevant health status and previous treatments related to chronic pain.
-
6.Utilize the checkboxes available for specific interventions requested, ensuring to select all appropriate options that apply to the patient’s situation.
-
7.In the comments section, add any additional notes or requirements necessary for the triage process to assist the receiving program.
-
8.Once all fields are complete, carefully review the entire form for any missing or incorrect information before finalizing it.
-
9.To finalize the form, ensure that the referring healthcare provider's signature is affixed in the designated area. This is crucial for the referral to be valid.
-
10.After completing the review, you can save your progress or download the completed form directly from pdfFiller. Choose the desired format for storage or printing.
-
11.To submit, follow the instructions related to your facility's procedures or coordinate with the chronic pain management program for the appropriate submission method.

Who is eligible to submit the Chronic Pain Management Program Referral Form?
The form can be submitted by certified healthcare providers in Ontario who are referring patients experiencing chronic pain to a management program.
Are there specific deadlines for submitting this referral form?
While there may be recommended timelines for patient referrals, specific deadlines can vary by program. It's best to check with the chronic pain management service for their guidelines.
What are the methods for submitting the referral form?
The completed form can typically be submitted via email, fax, or in person depending on the policies of the chronic pain management program. Verify with the program for preferred methods.
What supporting documents are required along with the referral form?
You may need to provide additional medical records, patient health assessments, or prior treatment documentation to support the referral. Check with the program for specific requirements.
What common mistakes should I avoid while filling out the form?
Ensure all fields are accurately completed and avoid leaving any mandatory sections blank. Also, verify that the referring provider's signature is included, as it's essential for processing.
How long does it take to process the Chronic Pain Management Program Referral Form?
Processing times can vary based on the chronic pain management program's workload. Typically, allowances of 5-10 business days are standard, but confirm with the program for precise timelines.
What if I have questions about the form while completing it?
If you have questions while filling out the form, consult the help documentation on pdfFiller or reach out to the healthcare provider's office for assistance about the referral process.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.