Last updated on Sep 9, 2014

Get the free Patient Information Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
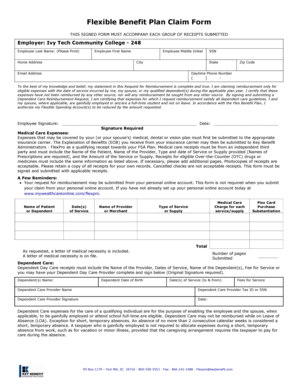
What is Patient Info Form
The Patient Information Form is a healthcare document used by providers to collect essential medical and personal details from patients.
pdfFiller scores top ratings on review platforms
Who needs Patient Info Form?
Explore how professionals across industries use pdfFiller.

Patient Info Form is needed by:
-
Patients seeking medical treatment
-
Healthcare providers during patient intake
-
Medical administrative staff for record-keeping
-
Insurance companies for processing claims
-
Family members assisting patients with healthcare forms
Comprehensive Guide to Patient Info Form
What is the Patient Information Form?
The Patient Information Form is a critical document in healthcare, encompassing various patient details necessary for effective health record management. This form includes essential patient demographics, medical history, and insurance information, enabling healthcare providers to maintain accurate health records. Signatures from patients are required to authorize the release of personal information and consent to treatment.
Completing this medical history form is vital for ensuring that healthcare professionals have a comprehensive understanding of a patient's health background, which directly influences patient care.
Purpose and Benefits of the Patient Information Form
This healthcare registration form serves multiple purposes in patient care and registration. Firstly, it facilitates the collection of crucial patient details needed by healthcare providers before a visit, promoting thorough assessment during consultations. Secondly, it helps assess the patient’s health history and personal context, which can lead to better-tailored treatment options.
Lastly, by streamlining the intake process, this form enhances overall patient care, ensuring that healthcare providers have accurate information at their fingertips.
Who Needs the Patient Information Form?
Different groups typically require this patient registration form for a variety of reasons. Patients seeking medical treatment at clinics or hospitals must fill out this form to provide their healthcare providers with necessary information. Additionally, healthcare providers rely on this comprehensive patient information to prepare for visits, helping ensure a more focused and informed healthcare experience.
It is essential for patients to understand their role in the registration process by providing accurate and complete information to facilitate efficient care.
How to Fill Out the Patient Information Form Online (Step-by-Step)
Filling out the Patient Information Form online is a straightforward process when using pdfFiller. Follow these steps:
-
Access the form through the pdfFiller website.
-
Begin with the "Patient Demographics" section, entering essential details like name, date of birth, and contact information.
-
Proceed to fill in the "Medical History" section, carefully detailing past illnesses or conditions.
-
Complete the "Insurance Details" field, ensuring all related information is accurate.
-
Review each section for accuracy before submission.
Taking the time to verify information maximizes the effectiveness and accuracy of the healthcare record.
Field-by-Field Instructions for the Patient Information Form
Understanding each field on the Patient Information Form is crucial for accurate completion. For instance, the "Name" field requires a full legal name, while the "Date of Birth" field should follow the format MM/DD/YYYY. Medical history may have multiple choice questions, requiring careful consideration of personal health history.
Checkboxes are typically used for gender selection, and it's vital to follow specified formats where necessary. Common mistakes include incomplete fields or inaccurate entries, which should be avoided by double-checking your responses.
Common Errors and How to Avoid Them
Frequent mistakes on the Patient Information Form can hinder the registration and care process. Common issues include leaving fields incomplete or providing incorrect information, which can lead to delays in treatment. To avoid these pitfalls:
-
Review the completed form thoroughly for accuracy.
-
Utilize pdfFiller’s tools for easy error correction and management.
-
Ensure all required fields are filled before submission.
Taking these precautions enhances the accuracy and efficiency of the registration process.
Submitting the Patient Information Form
Once the Patient Information Form is completed, submitting it correctly is essential. There are various options available:
-
Online submission through pdfFiller is the preferred method for convenience.
-
Printing and faxing the completed form is also an option if necessary.
-
Check if there are any submission fees that may apply.
Lastly, be aware of the timeline for processing after submission to understand when you can expect a response from healthcare providers.
Security and Compliance for the Patient Information Form
Security and compliance are paramount when submitting the Patient Information Form. pdfFiller employs robust security measures, including 256-bit encryption and adherence to HIPAA regulations. This ensures that sensitive patient information remains confidential and secure throughout the submission process.
Healthcare providers and patients alike must prioritize data privacy, acknowledging the importance of complying with existing healthcare regulations during the form submission process.
Witnessing the Importance of Accurate Patient Registration
Accurate completion of the Patient Information Form profoundly impacts healthcare outcomes. By providing complete and precise information, patients enable healthcare providers to deliver tailored care effectively. Utilizing pdfFiller simplifies this process, allowing users to fill out, edit, and securely submit their patient information forms online.
Efficient use of pdfFiller enhances the overall experience for both patients and providers, ensuring a smooth and effective healthcare journey.
How to fill out the Patient Info Form
-
1.To access the Patient Information Form on pdfFiller, visit the pdfFiller website and search for 'Patient Information Form.' Click on the form to open it in the editing interface.
-
2.Once the form is open, use the toolbar to navigate to different sections of the form. Each section has designated fields for entering information.
-
3.Before you start filling out the form, gather necessary information including personal identification, medical history, any family medical history, and insurance details if applicable.
-
4.Begin filling in the first section with your personal demographics. Provide your name, address, and contact information in the indicated fields.
-
5.Next, move to the medical history section. Input details about your past medical conditions and treatments. Use the checkboxes to indicate any relevant health issues.
-
6.Continue filling out the family medical history and personal history sections, ensuring all relevant information is accurately documented.
-
7.Complete the insurance information section by entering your insurance provider’s details, policy number, and any other required information.
-
8.After filling out all sections, thoroughly review the form to ensure accuracy and completeness. Look for any missing fields or unclear entries.
-
9.Once satisfied with your entries, save the form on pdfFiller by clicking the save icon. You can also download or print the filled form for your records.
-
10.To submit the form, follow the instructions provided by the healthcare provider or institution. If needed, you can email the completed form directly from pdfFiller.

Who is required to sign the Patient Information Form?
Patients are required to sign the Patient Information Form. This signature authorizes the healthcare provider to access the patient's medical information and facilitate treatment.
What information is typically required on the form?
The form generally requires personal demographics, medical history, family medical history, personal history, and insurance information to ensure accurate health records.
How can I submit the completed Patient Information Form?
Once completed, you may submit the form by following the instructions provided by your healthcare provider. Common methods include email, fax, or in-person submission.
What should I do if I make a mistake on the form?
If you make a mistake, you can easily edit the fields in pdfFiller. Double-check each section to ensure all information is correct before saving and submitting.
Is there a deadline for submitting the Patient Information Form?
While specific deadlines may vary by provider, it’s advisable to submit the form as soon as possible, preferably before your scheduled appointment.
Can a family member fill out the Patient Information Form on my behalf?
Yes, a family member can assist in filling out the form, particularly if the patient needs help understanding the questions or providing accurate information.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.