Last updated on Sep 5, 2014
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
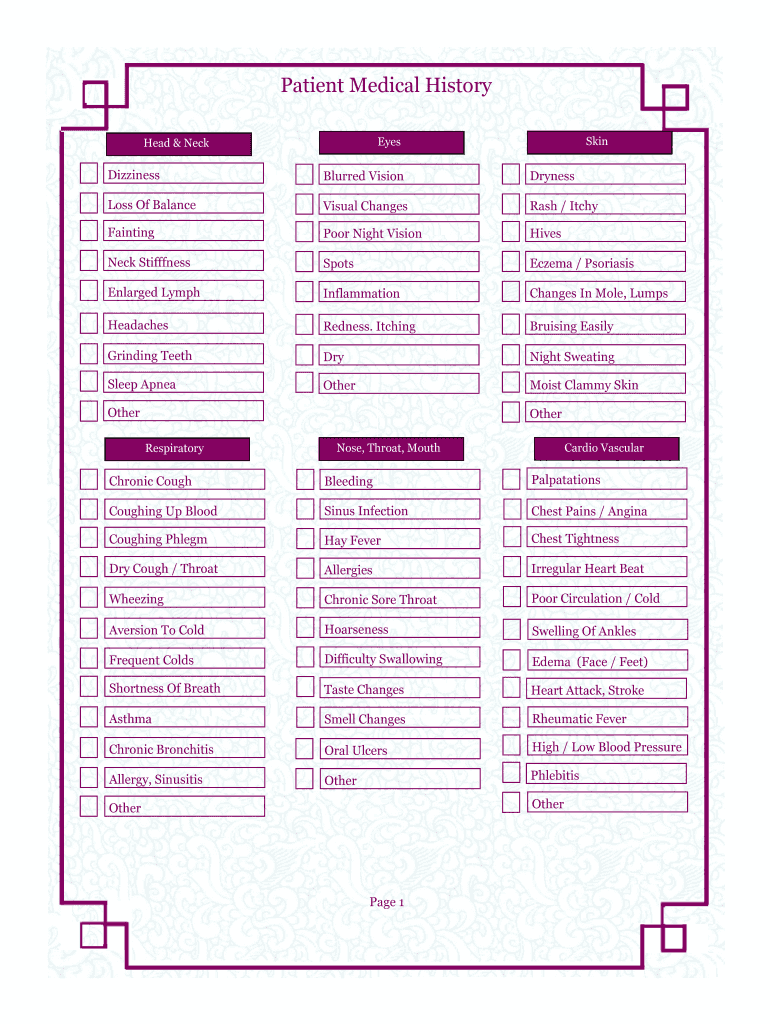
What is Medical History Form
The Patient Medical History Form is a healthcare document used by medical professionals to collect comprehensive medical history details from patients.
pdfFiller scores top ratings on review platforms
Who needs Medical History Form?
Explore how professionals across industries use pdfFiller.

Medical History Form is needed by:
-
Healthcare providers seeking patient information
-
Clinics implementing patient registration processes
-
Hospitals requiring detailed health records
-
Insurance companies assessing medical histories
-
Patients needing to document health conditions
-
Guardians assisting patients in completing forms
Comprehensive Guide to Medical History Form
What Is the Patient Medical History Form?
The Patient Medical History Form is a crucial document in healthcare settings, designed to gather comprehensive medical history from patients. This form is essential for accurate diagnosis and treatment, as it provides healthcare providers with insights into a patient's overall health and previous medical issues. Typically, the form is completed by patients themselves or by their guardians, allowing for detailed reporting of past illnesses and health concerns.
By collecting this information, healthcare professionals can make more informed decisions regarding diagnosis and treatment options.
Purpose and Benefits of the Patient Medical History Form
The primary purpose of the Patient Medical History Form is to facilitate a thorough understanding of a patient's health background and existing conditions. This form is instrumental in identifying potential health risks, particularly those that may arise from family medical history.
Additionally, it promotes better communication between patients and their doctors, ensuring that all relevant health issues are addressed. By utilizing this medical history template, professionals can improve patient care through informed assessments.
Key Features of the Patient Medical History Form
The Patient Medical History Form includes several key sections that make it structured and easy to navigate. These sections cover personal information, past illnesses, and family history, allowing for a comprehensive overview of the patient’s medical background.
-
Fillable fields for personal and medical information
-
Checkboxes for various symptoms
-
Accessible online via pdfFiller for easy completion
This well-organized format enables quick data entry and retrieval, ensuring that healthcare providers receive accurate information efficiently.
Who Needs to Fill Out the Patient Medical History Form?
The Patient Medical History Form is essential for various individuals involved in healthcare. Primarily, patients seeking medical treatment must complete this form to inform their healthcare providers about their health history. Additionally, guardians may need to fill out the form for minors or individuals who are incapacitated.
Healthcare professionals may also use this form to gather accurate patient data needed for effective diagnosis and treatment plans.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
Completing the Patient Medical History Form online through pdfFiller is simple and convenient. Follow these steps to fill out the form effectively:
-
Access the Patient Medical History Form on pdfFiller.
-
Fill in your personal and medical information accurately in the designated fields.
-
Utilize checkboxes to indicate any symptoms you may be experiencing.
-
Save your progress periodically to avoid losing information.
-
Review the form for any errors or omissions before submission.
Engaging with these interactive features ensures the submission of a comprehensive and error-free medical history form.
Review and Validation Checklist for Your Patient Medical History Form
Before submitting your Patient Medical History Form, it is essential to double-check the information provided. Use this checklist to ensure everything is in order:
-
Confirm all necessary fields are filled out completely.
-
Check for the accuracy of personal and medical information.
-
Look for common mistakes, such as omitted fields.
The importance of accuracy in submitting the medical history form cannot be underestimated, as it plays a significant role in your healthcare provider's ability to offer suitable care.
How to Securely Submit Your Patient Medical History Form
Submitting your Patient Medical History Form involves several options while ensuring your data is protected. You can choose to submit the form online, print it for physical submission, or fax it directly to your healthcare provider.
Security is paramount; pdfFiller employs 256-bit encryption and is fully HIPAA compliant to safeguard your sensitive information. If required, digital signing (eSigning) options are available, which maintain the security of your submission.
What Happens After You Submit Your Patient Medical History Form?
After submission, your Patient Medical History Form undergoes processing by your healthcare provider. Typically, medical offices will review the submission to extract important health information efficiently.
Response times may vary, but it is advisable to follow up with the provider for any necessary updates regarding appointments or further procedures.
Security and Privacy of Your Patient Medical History Information
The security of your Patient Medical History information is of utmost concern. Healthcare providers implement strict data encryption methods and adhere to compliance standards such as HIPAA and GDPR to protect user data. Utilizing secure platforms for handling sensitive documents is imperative.
Patients should also take steps to manage their personal health records safely, ensuring they are always stored in secure locations.
Streamline Your Patient Registration with pdfFiller
pdfFiller offers a seamless solution for completing your Patient Medical History Form. With capabilities to edit, fill, and eSign documents, pdfFiller enhances the user experience while ensuring the security of personal information.
By utilizing pdfFiller, you can efficiently manage your patient registration process, enabling healthcare providers to deliver timely and informed care.
How to fill out the Medical History Form
-
1.Access the Patient Medical History Form on pdfFiller by searching for its title in the search bar.
-
2.Select the form from the search results and open it in the pdfFiller editor.
-
3.Begin filling out the required fields by clicking on each blank area or checkbox.
-
4.Gather necessary information such as current and past health issues, pain symptoms, and family medical history before starting.
-
5.Make sure you have your identification and any previous medical records available for reference.
-
6.Navigate through the sections methodically, providing information on your medical history as accurately as possible.
-
7.Review the details you've entered carefully to ensure all information is correct and complete.
-
8.Utilize the save feature to avoid losing your progress, especially if you need to return to the form later.
-
9.Once the form is complete, you can download a copy, submit it to your healthcare provider directly through the platform, or save it for future reference.

Who should complete the Patient Medical History Form?
The Patient Medical History Form should be completed by patients or their guardians, providing detailed information about health conditions and family medical history to healthcare providers.
What information is required to fill out the form?
You will need details about your current and past health issues, symptoms, medications, allergies, and relevant family medical history to complete the form accurately.
How can I submit the completed form?
Once you finish filling out the Patient Medical History Form, you can submit it directly to your healthcare provider via pdfFiller or download it for printing and manual submission.
Are there any deadlines for submitting this form?
It’s important to submit the Patient Medical History Form before your scheduled appointment to ensure the healthcare provider has your information on hand for review.
What should I do if I make a mistake on the form?
If you make a mistake, you can easily edit the fields in pdfFiller. Review your entries and make necessary corrections before submitting the form.
Do I need to notarize the form?
No, the Patient Medical History Form does not require notarization. Simply complete and submit it to your healthcare provider.
How long does it take to process the form?
Processing time for the Patient Medical History Form can vary by provider, but typically it is reviewed during the patient’s appointment or shortly after submission.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.