CMS-L564 S 2016 free printable template
Show details
DEPARTMENT DE SALAD Y SERVICES HUMANS
CENT ROS DE SERVICES DE MEDICARE Y MEDICAIDFormulario Abroad
OMB No. 09380787SOLICITUD DE INFORMATION SORE EL TEMPLE
CUL ES EL PROPERTY DE ESTER FORMULA RIO?EU
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign CMS-L564 S
Edit your CMS-L564 S form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your CMS-L564 S form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit CMS-L564 S online



Follow the guidelines below to benefit from the PDF editor's expertise:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Upload a document. Select Add New on your Dashboard and transfer a file into the system in one of the following ways: by uploading it from your device or importing from the cloud, web, or internal mail. Then, click Start editing.
3
Edit CMS-L564 S. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Save your file. Choose it from the list of records. Then, shift the pointer to the right toolbar and select one of the several exporting methods: save it in multiple formats, download it as a PDF, email it, or save it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
CMS-L564 S Form Versions
Version
Form Popularity
Fillable & printabley
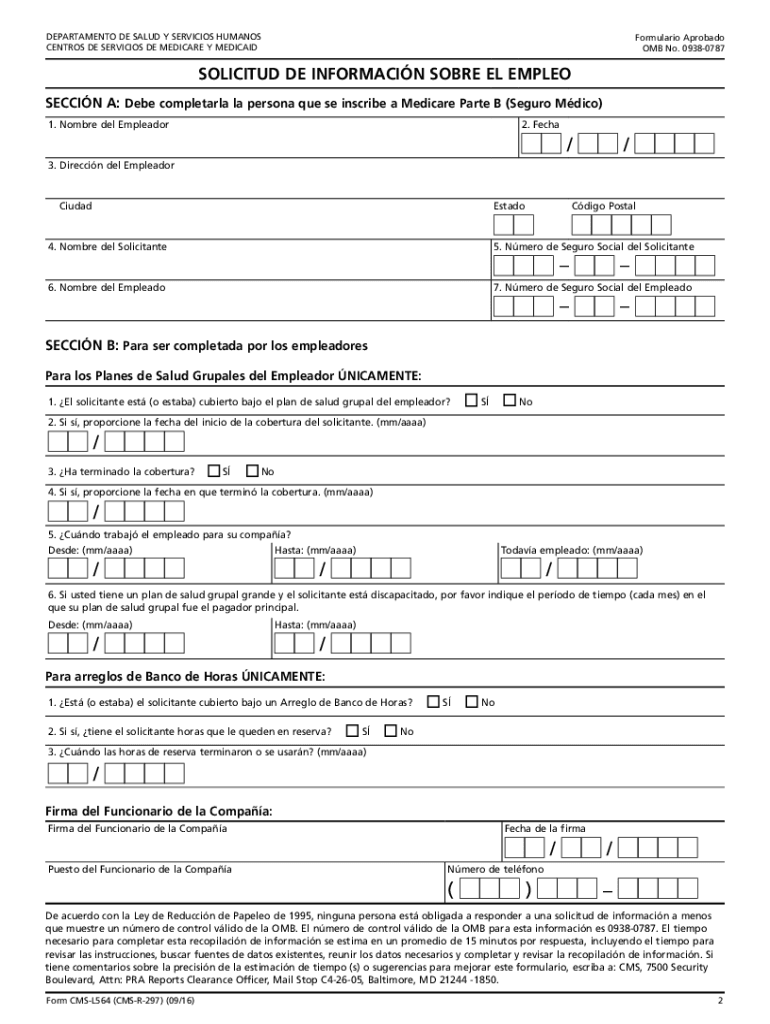
How to fill out CMS-L564 S
How to fill out CMS-L564 S
01
Download the CMS-L564 S form from the official CMS website.
02
Fill in the applicant's personal information, including name, address, and date of birth.
03
Provide information about the employer or union health coverage, including the name and address of the insurance provider.
04
Indicate the period of coverage you are requesting for by selecting appropriate start and end dates.
05
Ensure that the employer or insurer signs and dates the form to verify the coverage details.
06
Review all filled information for accuracy.
07
Submit the completed form to the Social Security Administration (SSA) or use it when applying for Medicare.
Who needs CMS-L564 S?
01
Individuals who are applying for Medicare based on their job-based health insurance coverage.
02
People who are eligible for Medicare but want to confirm their coverage period and details to avoid penalties.
Fill
form
: Try Risk Free
People Also Ask about
Can I submit form CMS L564 online?
You can complete the Part B SEP online or you can mail your completed CMS 40B, Application for Enrollment in Medicare - Part B (Medical Insurance) and CMS L564 - Request for Employment Information to your local Social Security office.
What forms do I need to fill out for Medicare Part B?
Fill out Form CMS-40B (Application for Enrollment in Medicare Part B). Send the completed form to your local Social Security office by fax or mail. Call 1-800-772-1213. TTY users can call 1-800-325-0778.
Who fills out CMS L564?
Form CMS-L564 is an employment information form from the Social Security Administration (SSA). It's used in conjunction with Form CMS-40B when you apply for Medicare part B during a special enrollment period (SEP). One portion is completed by you and the other is completed by your employer or your spouse's employer.
What is a CMS L564 form for spouse?
Form CMS-L564 is a form used by the Social Security Administration to grant a Special Enrollment Period to Medicare beneficiaries who initially turned down Part B coverage because they were receiving group health benefits from their employer or a spouse's employer.
Can form CMS L564 be submitted online?
You can complete the Part B SEP online or you can mail your completed CMS 40B, Application for Enrollment in Medicare - Part B (Medical Insurance) and CMS L564 - Request for Employment Information to your local Social Security office.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I send CMS-L564 S for eSignature?
To distribute your CMS-L564 S, simply send it to others and receive the eSigned document back instantly. Post or email a PDF that you've notarized online. Doing so requires never leaving your account.
How do I make changes in CMS-L564 S?
With pdfFiller, the editing process is straightforward. Open your CMS-L564 S in the editor, which is highly intuitive and easy to use. There, you’ll be able to blackout, redact, type, and erase text, add images, draw arrows and lines, place sticky notes and text boxes, and much more.
How do I edit CMS-L564 S on an Android device?
Yes, you can. With the pdfFiller mobile app for Android, you can edit, sign, and share CMS-L564 S on your mobile device from any location; only an internet connection is needed. Get the app and start to streamline your document workflow from anywhere.
What is CMS-L564 S?
CMS-L564 S is a form used by individuals to document and report their health coverage information to the Centers for Medicare & Medicaid Services (CMS) in order to determine eligibility for Medicare.
Who is required to file CMS-L564 S?
Individuals applying for Medicare who have health coverage and need to report this information to CMS are required to file CMS-L564 S.
How to fill out CMS-L564 S?
To fill out CMS-L564 S, individuals need to provide their personal information, details about their health coverage, and sign the form to certify the information provided is accurate.
What is the purpose of CMS-L564 S?
The purpose of CMS-L564 S is to verify and document an individual's health coverage status as part of the Medicare enrollment process.
What information must be reported on CMS-L564 S?
The information that must be reported on CMS-L564 S includes the individual's name, Medicare number, type of health coverage, and dates of coverage.
Fill out your CMS-L564 S online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
CMS-l564 S is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
