Last updated on Oct 5, 2014
Get the free Authorization for Disclosure of Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Health Info Disclosure
The Authorization for Disclosure of Health Information is a healthcare form used by patients to authorize the release of their health information to specified healthcare providers or plans.
pdfFiller scores top ratings on review platforms
Who needs Health Info Disclosure?
Explore how professionals across industries use pdfFiller.

Health Info Disclosure is needed by:
-
Patients seeking medical records
-
Healthcare providers requesting patient consent
-
Insurance companies for claim processing
-
Attorneys involved in medical cases
-
University health services for student records
-
Family members assisting patients
-
Mental health professionals managing patient care
Comprehensive Guide to Health Info Disclosure
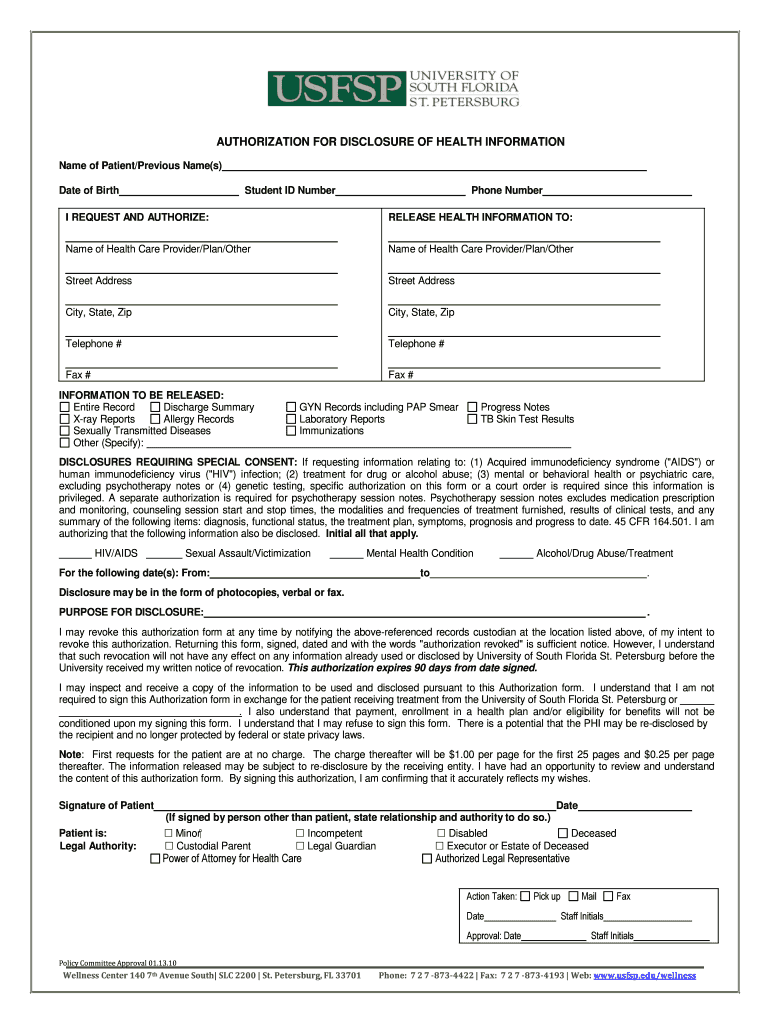
What is the Authorization for Disclosure of Health Information?
The Authorization for Disclosure of Health Information form is a crucial document designed for patients to permit the release of their health information to specified healthcare providers. This form plays a vital role in ensuring that patients have control over their medical data while facilitating necessary communication between healthcare entities. Associated with the University of South Florida St. Petersburg, the form is commonly used in various healthcare settings, emphasizing the importance of patient authorization in health information management.
Purpose and Benefits of the Authorization for Disclosure of Health Information
This form is essential for maintaining patient rights concerning their health information. By formalizing consent, it offers numerous advantages, including:
-
Enhanced control for patients over who has access to their medical records.
-
Protection of patient privacy by ensuring that sensitive information is shared only with authorized individuals.
-
The ability to navigate complex healthcare situations, especially when multiple providers are involved.
Understanding the importance of consent is critical in sensitive health-related disclosures, empowering patients to manage their data effectively.
Key Features of the Authorization for Disclosure of Health Information
The Authorization for Disclosure of Health Information form contains several key features that users should be aware of, including:
-
Fields for personal information such as Patient Name, Date of Birth, and Student ID Number.
-
Optional checkboxes for sensitive information, including HIV/AIDS and Mental Health.
-
Special consent requirements and signature fields that validate the authorization.
These features help ensure that all necessary information is collected to comply with privacy regulations.
Who Needs the Authorization for Disclosure of Health Information?
This form is required for individuals who need to share their medical records with others. Patients requesting to transfer their health information to different healthcare providers or to receive care from multiple providers should fill out this form. Additionally, university students utilizing healthcare services associated with the University of South Florida St. Petersburg are often in need of this authorization to share relevant medical details.
How to Fill Out the Authorization for Disclosure of Health Information Online (Step-by-Step)
Filling out the Authorization for Disclosure of Health Information through pdfFiller is straightforward. Follow these steps:
-
Access the form through the pdfFiller platform.
-
Enter your personal details, including your name, date of birth, and student ID number.
-
Select any sensitive information types via checkboxes, if applicable.
-
Sign the form digitally using the eSignature feature.
-
Review all entries to ensure accuracy before submission.
By adhering to these steps, users can efficiently and securely complete the form online.
Security and Compliance for the Authorization for Disclosure of Health Information
Users can rest assured that their information is safe when using the Authorization for Disclosure of Health Information. pdfFiller employs advanced security measures, including 256-bit encryption and adherence to HIPAA compliance. Patients retain the right to revoke their authorization at any time, allowing them to manage their health information actively. Furthermore, the platform maintains clear record retention policies to safeguard your data throughout its lifecycle.
Submission Methods and What Happens After You Submit the Authorization for Disclosure of Health Information
Submitting the Authorization for Disclosure of Health Information can be done through various methods. Users may choose to submit online, via email, or in person at the designated office. After submission, it is important to confirm the receipt of the form and track the request status. Typically, patients can expect a timeline for receiving outcomes from the request, ensuring transparency throughout the process.
Common Errors and How to Avoid Them While Filling Out the Form
While completing the Authorization for Disclosure of Health Information, users may encounter common pitfalls. Avoid these mistakes by:
-
Double-checking all entries for accuracy before submitting the form.
-
Ensuring that all required fields are filled out completely.
-
Validating sensitive information against the specific requirements outlined in the form.
Taking these precautions can significantly reduce errors and enhance the approval process.
Sample of a Completed Authorization for Disclosure of Health Information
Referencing a sample of a completed Authorization for Disclosure of Health Information can greatly assist users. A filled-out form should include:
-
Patient's name and date of birth clearly printed.
-
Accurate completion of sensitive information checkboxes, if applicable.
-
A visible signature validating the authorization.
This visual guide serves as an effective reference to enhance accuracy during the form-filling process.
Maximize Your Experience with pdfFiller
Using pdfFiller to fill out the Authorization for Disclosure of Health Information offers numerous advantages. With its user-friendly interface, patients can easily navigate the form completion process. Security and compliance are prioritized, providing peace of mind while managing sensitive documents. Additionally, users can explore various editing, eSigning, and sharing tools available on the platform to enhance their document management experience.
How to fill out the Health Info Disclosure
-
1.To begin, access pdfFiller and search for the 'Authorization for Disclosure of Health Information' form using the search bar.
-
2.Once located, select the form to open it in the editor. Familiarize yourself with the layout and available fields on pdfFiller.
-
3.Collect necessary personal information including your name, date of birth, and if applicable, your Student ID Number. This information is crucial for completing the form accurately.
-
4.Start filling in the required fields. Enter your name in the designated area marked 'Name of Patient' and provide your date of birth in the respective field.
-
5.If applicable, input your Student ID Number in the provided section for those affiliated with academic institutions.
-
6.For sensitive information, utilize the checkboxes to authorize the disclosure of specific types of health information such as HIV/AIDS or Mental Health Condition.
-
7.Carefully read the instructions and ensure you understand the statement: 'I REQUEST AND AUTHORIZE.' This confirms your consent.
-
8.Sign the form in the area provided for 'Signature of Patient.' Ensure your signature reflects your agreement and consent.
-
9.Once all fields are completed, review the form for accuracy. Check that all personal information and selections are correct before proceeding.
-
10.Save your completed form by clicking on the save icon. You may also choose to download a copy to your device or submit it directly through pdfFiller's submission options.

Who is eligible to use the Authorization for Disclosure of Health Information form?
Any patient who wishes to authorize the release of their health information to healthcare providers or plans is eligible to use this form. It is particularly relevant for individuals seeking to share their medical records.
Is there a deadline for submitting this authorization form?
The Authorization for Disclosure of Health Information does not typically have a specific deadline. However, it should be submitted as soon as you need your records or wish to authorize disclosure to ensure timely processing.
How can I submit the completed authorization form?
You can submit the completed form directly through pdfFiller, which offers submission options, or download it and deliver it in-person or via mail to the required healthcare provider.
What supporting documents are required when submitting the form?
Supporting documents are usually not required for the authorization form itself; however, it may be helpful to include a valid ID or other identifying information to facilitate the release of records.
What common mistakes should I avoid when filling out the form?
Be sure to fill out all required fields completely and accurately. A common mistake is forgetting to sign the form, as an unsigned authorization is typically not valid. Double-check your selections regarding sensitive information as well.
How long does it take to process the authorization form?
Processing times may vary depending on the healthcare provider or institution receiving the form. Generally, it's advisable to allow several days to a couple of weeks for processing.
What should I do if I need to revoke my authorization?
If you wish to revoke your authorization, you need to contact the healthcare provider or institution that received the form directly. It's recommended to submit a written request outlining your decision to revoke consent.
Related Forms



Get the latest insights from our blog
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.