Last updated on Apr 10, 2026

Get the free Authorization for Disclosure of Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is authorization for disclosure of
The Authorization for Disclosure of Medical Information is a legal document used by patients or their representatives to permit the release of protected health information to specified third parties.
pdfFiller scores top ratings on review platforms
Who needs authorization for disclosure of?
Explore how professionals across industries use pdfFiller.

Authorization for disclosure of is needed by:
-
Patients seeking medical treatment authorization
-
Parents or guardians managing health information for minors
-
Legal representatives handling patient consent
-
Healthcare providers requiring patient consent for release
-
Military personnel utilizing TRICARE services
-
Administrators of Military Treatment Facilities
Comprehensive Guide to authorization for disclosure of
What is the Authorization for Disclosure of Medical Information?
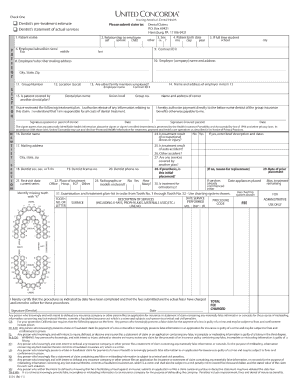
The Authorization for Disclosure of Medical Information is a critical form, specifically the DD Form 2870, designed to facilitate the release of a patient's protected health information to authorized third parties. This form is essential for Military Treatment Facilities, Dental Treatment Facilities, and TRICARE Health Plans to ensure proper handling and sharing of medical data. The form requires specific details including the patient's identity and the nature of the medical information being disclosed.
Understanding the role of the DD Form 2870 is vital for patients, as improper completion can lead to delays in accessing necessary medical services or insurance claims. Therefore, it is imperative that users are familiar with this medical information release form and adhere to the guidelines when filling it out.
Purpose and Benefits of the Medical Information Disclosure Authorization
The primary purpose of the medical information disclosure authorization is to protect patient health information while allowing the necessary sharing of information between healthcare providers and third parties. This form ensures that patients have control over their personal medical information, reinforcing the importance of patient consent and privacy.
Benefits of completing this authorization include improved communication between healthcare providers and the timely processing of insurance claims, which ultimately enhances patient care. By obtaining consent, healthcare providers can access essential information required for effective treatment.
Who Needs the Authorization for Disclosure of Medical Information?
Individuals who typically need to complete the Authorization for Disclosure of Medical Information include patients, parents, and legal representatives. Each role plays a crucial part in the authorization process, ensuring that the right parties have access to necessary medical information.
There are specific scenarios in which this disclosure is vital, such as during medical treatment or filing insurance claims. Proper authorization helps streamline these processes and ensures legal compliance regarding patient health information disclosure.
How to Fill Out the Authorization for Disclosure of Medical Information Online
Completing the DD Form 2870 online involves a few step-by-step procedures to ensure accuracy and compliance:
-
Access the form and begin by entering personal data such as the patient's full name and date of birth.
-
Fill in the treatment details, specifying which medical information is being shared and for what purpose.
-
Ensure that the form is signed and dated properly by the patient or their legal representative.
Careful attention to each field is critical for the successful submission of the military medical release form.
Common Errors and How to Avoid Them When Filling Out the Form
Many users encounter common errors that can delay the processing of the Authorization for Disclosure of Medical Information. Frequent mistakes include:
-
Incomplete fields, which can lead to rejections.
-
Incorrect signatures or missing dates, which are essential for validation.
To avoid these issues, users should perform validation checks prior to submission, ensuring all necessary information is accurately provided.
Security and Compliance for the Authorization for Disclosure of Medical Information
When handling sensitive personal data, security and compliance are of utmost importance. The Authorization for Disclosure of Medical Information complies with standards such as HIPAA and GDPR, ensuring that patient data is handled responsibly.
pdfFiller implements robust security measures, including 256-bit encryption and adherence to SOC 2 Type II protocols, protecting personal health information throughout the document handling process. Understanding these measures reassures users that their data remains safe and secure.
How to Submit the Authorization for Disclosure of Medical Information
Submitting the Authorization for Disclosure of Medical Information can be done in several ways. Users may choose between:
-
Online submission through authorized platforms for timely processing.
-
Traditional mailing methods for those who prefer paper submissions.
It's important to identify the correct destination and relevant contacts for submission, ensuring the form reaches the appropriate department without delay.
What Happens After You Submit the Authorization for Disclosure of Medical Information?
Once the Authorization for Disclosure of Medical Information is submitted, users can track their application status through various channels. This allows them to confirm whether their submission was received and is being processed.
Users may experience different outcomes post-submission, such as receiving further communication regarding additional information or approval timelines for their authorization request. Understanding these steps helps manage expectations effectively.
How pdfFiller Can Help with Your Authorization for Disclosure of Medical Information
Utilizing pdfFiller offers several advantages for filling out the DD Form 2870. This platform provides features that enhance efficiency such as:
-
Easy form filling through an intuitive interface, allowing for quick completion.
-
Secure document sharing, ensuring privacy while collaborating with healthcare providers.
-
eSigning capabilities that simplify the signing process, making it faster and more reliable.
Employing pdfFiller can significantly streamline the process of managing your military medical release form.
How to fill out the authorization for disclosure of
-
1.To start, visit pdfFiller and search for 'Authorization for Disclosure of Medical Information' to access the form.
-
2.Once opened, review the form's top instructions for guidance on filling it out correctly.
-
3.Begin by entering the patient's personal details, including their name, date of birth, and contact information in the specified fields.
-
4.Next, identify the specific healthcare provider or facility that the information will be disclosed to by filling in their details.
-
5.In the section pertaining to the treatment details, ensure to describe the type of medical information you wish to authorize for release.
-
6.Specify the purpose for the disclosure clearly in the designated field, such as ongoing treatment or legal matters.
-
7.Check all relevant boxes and fields as required to collect the necessary consent for information sharing.
-
8.Review the completed form for any missing information or errors before signing.
-
9.If you're the patient, sign and date the form in the appropriate sections. If you are a representative, include your capacity or relationship to the patient.
-
10.After final review, you can save the completed form locally or choose to download it as a PDF.
-
11.Finally, follow the specific submission instructions provided by the relevant healthcare facility or the entity requesting the disclosure.

Who is eligible to fill out this form?
The Authorization for Disclosure of Medical Information can be filled out by patients, parents or legal guardians of minors, and legal representatives acting on behalf of the patient.
What documents are required to complete the form?
Generally, you will need personal identification, such as a driver’s license, and any relevant medical records or information about the treatment for which you’re authorizing disclosure.
How do I submit the completed form?
After filling out the form, submit it as instructed by the requesting healthcare provider. This could involve mailing it, emailing a scanned copy, or delivering it in person.
Are there any deadlines for submitting this form?
While there may not be strict deadlines, it is advised to complete and submit the form as soon as possible, especially if it relates to scheduled medical services.
What common mistakes should be avoided?
Ensure all requested fields are filled out completely and signed. Omitting information or failing to obtain necessary signatures can delay processing or invalidate the form.
How long does it take for processing of this authorization?
Processing times can vary depending on the facility. Typically, once submitted, it may take several days to a couple of weeks for your authorization to be acted upon.
Can I revoke this authorization once it is submitted?
Yes, the authorization can be revoked at any time by notifying the healthcare provider in writing. Make sure to obtain instructions on how to do this to ensure your wishes are followed.
Related Forms




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.