Last updated on Oct 31, 2014
Get the free Medical Care Reimbursement Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medical Reimbursement Form
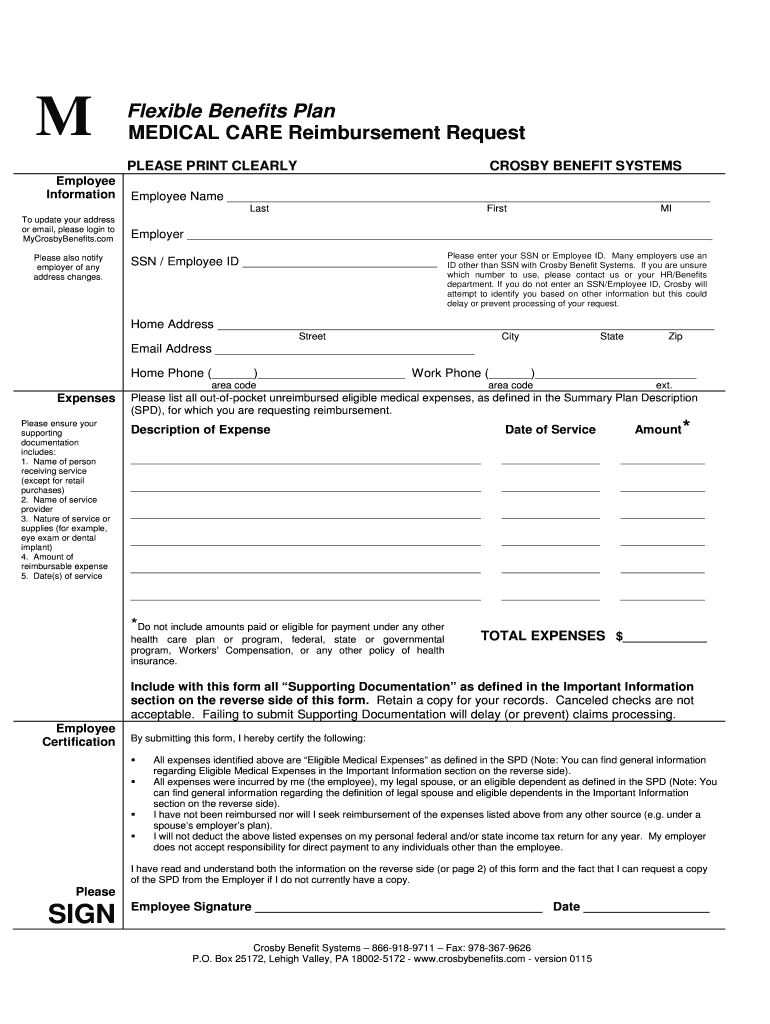
The Medical Care Reimbursement Request Form is a healthcare document used by employees to request reimbursement for out-of-pocket medical expenses not covered by other health plans.
pdfFiller scores top ratings on review platforms
Who needs Medical Reimbursement Form?
Explore how professionals across industries use pdfFiller.

Medical Reimbursement Form is needed by:
-
Employees seeking reimbursement for medical expenses.
-
HR personnel managing employee benefits.
-
Insurance administrators processing claims.
-
Benefit coordinators at Crosby Benefit Systems.
-
Healthcare providers verifying patient expenses.
Comprehensive Guide to Medical Reimbursement Form
What is the Medical Care Reimbursement Request Form?
The Medical Care Reimbursement Request Form is an essential document used by employees to request reimbursement for out-of-pocket medical expenses that are not covered by their health plans. This form is primarily utilized by employees seeking to reclaim costs incurred during medical services, ensuring they receive the financial support they deserve. Common situations requiring this form include expenses related to prescriptions, medical treatments, or other healthcare-related costs.
Purpose and Benefits of the Medical Care Reimbursement Request Form
The primary purpose of the Medical Care Reimbursement Request Form is to facilitate the process through which employees can reclaim eligible medical expenses. By using this form, employees can effectively navigate the financial burdens of healthcare. Furthermore, the form provides significant benefits for employers, as it streamlines reimbursement processes and promotes employee satisfaction. Employees facing medical costs can also leverage this form for personal finance management, making it a valuable tool in their financial toolkit.
Key Features of the Medical Care Reimbursement Request Form
This form is designed with several key features that ensure the reimbursement process is straightforward and efficient. Essential fields include:
-
Employee name
-
Social Security Number (SSN)
-
Service provider details
-
Expense amount
-
Date of service
Additionally, the fillable nature of the form allows for easy completion and submission. Supporting documentation, such as receipts, is necessary for processing. The signature of the employee is required to validate the request before submission.
Who Needs the Medical Care Reimbursement Request Form?
Eligibility to utilize the Medical Care Reimbursement Request Form typically includes employees who have incurred eligible medical expenses. This can encompass full-time, part-time, and even temporary employees depending on company policies. Situations that necessitate the use of this form include various healthcare services ranging from routine check-ups to emergency medical treatments.
How to Fill Out the Medical Care Reimbursement Request Form Online (Step-by-Step)
Filling out the Medical Care Reimbursement Request Form online is simple and efficient when using pdfFiller. Follow these steps for a seamless submission:
-
Access the form on pdfFiller.
-
Enter your personal information, including your name and SSN.
-
Provide details about the medical service received, including the provider's name.
-
Clearly state the amount you are claiming.
-
Attach any necessary documentation, such as receipts.
-
Review the information for accuracy before submission.
Collecting accurate expense data upfront will facilitate a smoother reimbursement experience.
Common Errors and How to Avoid Them When Submitting the Form
Employees often encounter common mistakes when completing the Medical Care Reimbursement Request Form, which can delay processing. Some frequent errors include:
-
Incomplete fields.
-
Missing signatures.
-
Incorrect or unclear documentation.
To avoid these pitfalls, validate the entered information carefully before submitting. Ensuring all details are accurate is crucial for timely reimbursement.
Submission Methods for the Medical Care Reimbursement Request Form
The completed Medical Care Reimbursement Request Form can be submitted using various methods, ensuring flexibility for all employees. Preferred submission methods recommended by Crosby Benefit Systems include:
-
Electronic submission via pdfFiller.
-
Mailing a printed copy.
Tracking your submission and confirming receipt with Crosby Benefit Systems is advisable to ensure your request is processed without delay.
What Happens After You Submit the Medical Care Reimbursement Request Form?
After submission, employees can expect a processing timeline that varies based on the complexity of the claim. Employees have the ability to check the status of their application by contacting Crosby Benefit Systems directly. Understanding potential outcomes, as well as knowing how to address issues that may arise, is essential for managing your reimbursement effectively.
Security and Compliance When Using the Medical Care Reimbursement Request Form
When submitting the Medical Care Reimbursement Request Form online, data protection is paramount. pdfFiller ensures that all submissions are secure through stringent measures, including 256-bit encryption and compliance with HIPAA regulations. This commitment to security guarantees that sensitive medical information is handled with the utmost care.
Enhance Your Experience with pdfFiller for the Medical Care Reimbursement Request Form
Utilizing pdfFiller for the Medical Care Reimbursement Request Form enhances your experience by providing an efficient platform for creating, filling out, and managing the form. The ease of editing and the benefits of a cloud-based solution allow you to handle your medical reimbursement requests with confidence. Explore additional document management and eSigning features to optimize your workflow.
How to fill out the Medical Reimbursement Form
-
1.Access the Medical Care Reimbursement Request Form on pdfFiller by searching for the form name in the platform's document library.
-
2.Open the form to view the blank fields and instructions. Utilize the toolbar to navigate easily through the document.
-
3.Before starting, gather necessary information including service details, provider names, expense amounts, and dates of service.
-
4.Fill out the Employee Name, SSN/Employee ID, and ensure your details are accurate. Proceed to fill in the expense details including the nature of the service and the amount.
-
5.Use pdfFiller's features to upload supporting documents such as bills and receipts by selecting the upload option.
-
6.Carefully review all filled fields for accuracy. Make sure you have signed the form, adding the date as required.
-
7.Once completed, save your work. You can download a copy of the form for your records or submit it directly through pdfFiller.

Who is eligible to use the Medical Care Reimbursement Request Form?
Employees who incur out-of-pocket medical expenses not covered by other health plans are eligible to use this form for reimbursement.
What supporting documents are needed to submit this form?
When submitting the Medical Care Reimbursement Request Form, be sure to include all relevant supporting documents, such as receipts, invoices, and proof of payment for the medical expenses.
How do I submit the Medical Care Reimbursement Request Form?
You can submit the completed form through pdfFiller by following the submission process outlined on the platform, which often includes electronic submission options.
Are there any deadlines for submitting this reimbursement request?
While the form metadata does not specify a deadline, it is best practice to submit your requests for reimbursement as soon as possible after incurring the expenses.
What common mistakes should I avoid when filling out this form?
Ensure that all fields are filled out accurately, especially the employee name and signature. Also, verify that your supporting documents are complete and correctly matched to the listed expenses.
How long will it take to process my reimbursement request?
Processing times can vary, but it typically takes a few weeks. Check with Crosby Benefit Systems for precise timelines regarding your claim.
Do I need to notarize the Medical Care Reimbursement Request Form?
No, notarization is not required for the Medical Care Reimbursement Request Form.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.