Last updated on Apr 10, 2026
Get the free Patient Information Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient information form
The Patient Information Form is a medical document used by healthcare providers to collect important personal and medical information from patients.
pdfFiller scores top ratings on review platforms
Who needs patient information form?
Explore how professionals across industries use pdfFiller.

Patient information form is needed by:
-
Patients seeking medical treatment
-
Healthcare providers for patient records
-
Insurance companies for billing purposes
-
Hospitals during patient admission
-
Clinics for patient intake processes
-
Medical administrative staff managing registrations
Comprehensive Guide to patient information form
What is the Patient Information Form?
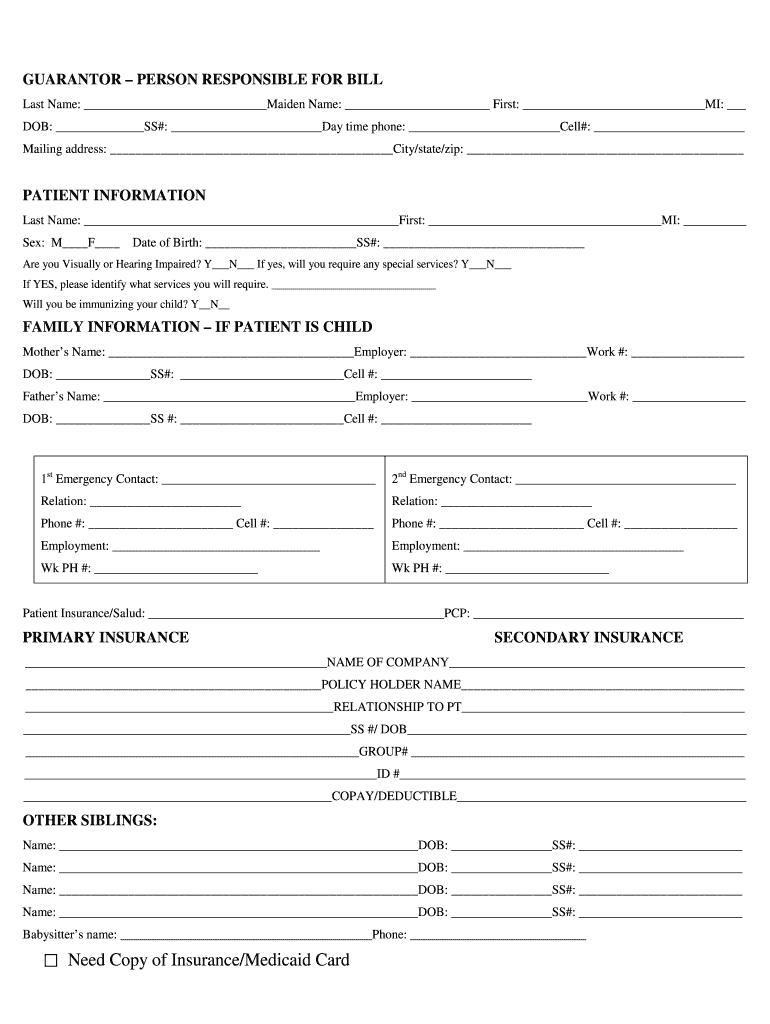
The Patient Information Form is a crucial tool used in healthcare settings to collect and maintain accurate medical records. This form includes various components such as personal information, medical history, and insurance details, which are essential for ensuring comprehensive patient care.
Accurate records significantly enhance the efficiency of healthcare operations and billing processes. By providing detailed medical history and personal data, patients can help healthcare providers deliver appropriate treatments and services.
Benefits of Using the Patient Information Form
Utilizing the Patient Information Form improves both patient registration and overall healthcare processes. This form streamlines patient intake, facilitating efficiency in operations and allowing healthcare staff to focus on providing quality care.
Additionally, accurate information aids in billing and insurance processing, reducing potential errors and delays. Furthermore, the proper use of this form enhances communication between patients and healthcare providers, leading to better patient outcomes.
Key Features of the Patient Information Form
The Patient Information Form includes essential fields such as last name, first name, date of birth, and social security number. With fillable checkboxes and clear instructions, it guides users in providing the necessary information efficiently.
Security is paramount in handling sensitive patient information, and this form incorporates robust measures to protect data integrity. Users can trust that their information remains confidential and secure throughout the collection process.
Who Should Use the Patient Information Form?
This form is beneficial for a variety of users, primarily targeting healthcare providers, clinics, and hospitals that require detailed patient data. Patients preparing for medical appointments will also find this form essential for sharing necessary information with their healthcare team.
By catering to both providers and patients, this patient intake form plays a vital role in facilitating effective healthcare delivery.
How to Fill Out the Patient Information Form Online (Step-by-Step)
-
Access the Patient Information Form through pdfFiller.
-
Carefully complete each field, entering personal and medical details as required.
-
Utilize the fillable checkboxes where applicable to ensure all necessary options are selected.
-
Double-check your information for accuracy before submission.
-
Follow the prompts to submit the form once completed.
Submission Methods and Delivery of the Patient Information Form
Users have several digital submission options for the completed Patient Information Form. Submissions can be made directly via pdfFiller, allowing for immediate processing.
Alternatively, users may choose to print the form and submit it through traditional channels such as mail or in-person delivery. Timely submission is critical, as it ensures that patients receive prompt access to the healthcare services they need.
Common Errors and How to Avoid Them
When completing the Patient Information Form, users may encounter common errors that can impact the accuracy of medical records. Frequent mistakes include incorrect personal details, incomplete fields, and overlooked checkboxes.
To minimize these errors, it is advisable to double-check all information before submission. Recognizing the consequences of inaccuracies in medical records can motivate users to be diligent when filling out the form.
Security and Privacy of Your Patient Information
pdfFiller prioritizes the security of your patient data while using its platform. The service implements 256-bit encryption and adheres to HIPAA and GDPR compliance standards to safeguard personal information.
Users can confidently manage their completed forms, knowing that privacy is upheld throughout the process. It is critical to handle sensitive documents responsibly to ensure their security.
Why Choose pdfFiller for Your Patient Information Form?
pdfFiller provides a user-friendly interface that simplifies the editing and filling of forms. With cloud-based access, users can fill out the Patient Information Form from anywhere, making it convenient for busy patients and healthcare providers alike.
The platform also features easy eSigning capabilities, allowing for a seamless completion process. With millions of satisfied users, pdfFiller has established itself as a trusted platform for handling medical forms.
Get Started with Your Patient Information Form Today
Begin your journey toward organized health records by accessing the Patient Information Form on pdfFiller. Leveraging the features of this platform will provide you with an efficient and effective experience in completing your healthcare documentation.
Accurate and well-structured health records are invaluable in ensuring that you receive the best possible care from your healthcare providers.
How to fill out the patient information form
-
1.To access the Patient Information Form on pdfFiller, visit the website and search for the form by its name or use the provided link from the healthcare provider.
-
2.Once located, click on the form to open it in pdfFiller's editing interface.
-
3.Familiarize yourself with the fillable fields, including personal details such as first name, last name, date of birth, and social security number.
-
4.Ensure you gather all necessary information, including insurance details, emergency contacts, and any relevant medical history, before starting to fill out the form.
-
5.Click on each field to enter data, making sure to double-check the accuracy of the entered information.
-
6.Use the guidelines and descriptions available within the form to complete all required fields, as some may be mandatory for submission.
-
7.After filling out the form, thoroughly review all provided information for accuracy and completeness.
-
8.Once reviewed, finalize the form by clicking the save button to ensure your data is recorded.
-
9.You can then download the form or submit it directly through pdfFiller, following the instructions provided on the platform.

Who needs to complete the Patient Information Form?
Any patient seeking medical treatment, as well as their caregivers, should complete the Patient Information Form to ensure that healthcare providers have accurate medical records and billing information.
What information do I need to fill out the form?
You will need your personal details such as your name, date of birth, social security number, address, and insurance information, as well as any medical history that may be relevant.
How do I submit the Patient Information Form?
You can submit the Patient Information Form via pdfFiller by either downloading the completed document and handing it in to your healthcare provider or using the online submission options if available.
Are there any common mistakes to avoid when filling out this form?
Ensure all required fields are completed, double-check for typographical errors, and provide up-to-date insurance information to avoid delays in processing your form.
How long does it take to process the Patient Information Form?
Processing time can vary depending on the healthcare provider's policies, but generally, you should allow a few days for your information to be updated in their system.
Is there a deadline for submitting the Patient Information Form?
It is best to submit the Patient Information Form as soon as possible before your appointment to ensure all records are prepared in advance.
Do I need any supporting documents to complete this form?
While the Patient Information Form primarily requires personal and medical details, you may need to provide supporting documents such as insurance cards or identification, depending on the provider's requirements.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.