Last updated on Apr 10, 2026

NY Affinity Health Plan Prior Authorization free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
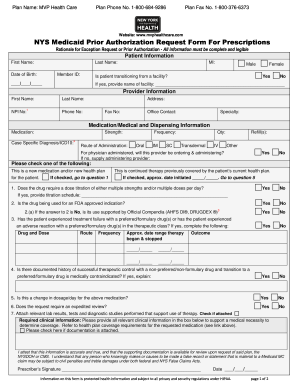
What is NY Affinity Health Plan Prior Authorization
The Prior Authorization Pharmacy Benefit Request Form is a healthcare document used by prescribers to request prior authorization for medication coverage from health plans in New York.
pdfFiller scores top ratings on review platforms
Who needs NY Affinity Health Plan Prior Authorization?
Explore how professionals across industries use pdfFiller.

NY Affinity Health Plan Prior Authorization is needed by:
-
Healthcare providers in New York
-
Prescribers requiring medication authorization
-
Pharmacists needing prior authorization
-
Patients seeking medication coverage
-
Health plans reviewing medication requests
Comprehensive Guide to NY Affinity Health Plan Prior Authorization
What is the Prior Authorization Pharmacy Benefit Request Form?
The Prior Authorization Pharmacy Benefit Request Form is a crucial document used by healthcare providers in New York to request prior authorization for medication coverage from health plans. This form gathers essential patient and provider information, ensuring that the healthcare process runs smoothly.
It is significant in the healthcare system as it helps secure necessary medication coverage, providing patients with timely access to their prescriptions. Using the prior authorization pharmacy form, providers can streamline their requests, avoiding unnecessary delays while navigating the intricacies of New York health plan form requirements.
Purpose and Benefits of the Prior Authorization Form
The primary purpose of the prior authorization form is to assist healthcare providers in obtaining medication approvals efficiently. By utilizing this medication authorization form, healthcare providers can adhere to compliance standards set by health plans, enhancing their operational efficiency.
Moreover, this form plays a crucial role in mitigating access delays to medications for patients. A well-completed medication authorization form not only expedites processing but also minimizes the chances of denials from health plans.
Key Features of the Prior Authorization Pharmacy Benefit Request Form
The layout of the Prior Authorization Pharmacy Benefit Request Form is user-friendly, featuring multiple fillable fields and explicit instructions that guide healthcare providers in completing the document accurately.
-
Mandatory sections include patient information, prescriber details, and medication specifics.
-
Signatures from the prescriber are required to validate the request.
-
Supporting documents, such as lab results, may also need to be submitted.
Providers can choose between electronic and paper submission options, facilitating flexibility in how they handle the medical necessity request form process.
Who Needs to Use the Prior Authorization Pharmacy Benefit Request Form?
Primary users of the prior authorization pharmacy benefit request form include prescribers, healthcare providers, and pharmacists. This form becomes essential in specific situations, particularly when medications fall under certain conditions or require prior authorization approvals.
Both healthcare providers and patients play crucial roles in this process, as their cooperation can significantly enhance the chances of successful authorization with the New York medical consent form.
Eligibility Criteria and State-Specific Rules
Eligibility for prior authorization varies and requires patients and medications to meet specific criteria. It is crucial to understand the regulations established in New York that dictate how the form should be completed.
-
Patients must have a valid prescription and medical justification for the requested medication.
-
Healthcare providers must be familiar with local health plan policies for effective submissions.
Proper knowledge of these requirements ensures a higher likelihood of approval for the pharmacy benefit request template.
How to Fill Out the Prior Authorization Pharmacy Benefit Request Form Online
Completing the prior authorization pharmacy benefit request form online can be streamlined through tools like pdfFiller. To assist users, here’s a step-by-step guide:
-
Gather necessary patient information including name, date of birth, and insurance details.
-
Complete the prescriber information section accurately.
-
Fill in medication details along with diagnosis codes supporting the request.
-
Review the form thoroughly for accuracy.
Common pitfalls to avoid include misrepresentation of patient information and neglecting to include required signatures, which can result in processing delays.
Submission Methods and What Happens After You Submit
There are several ways to submit the completed prior authorization pharmacy benefit request form, including online submission, mailing, or in-person delivery. Understanding these methods is essential for expeditious processing.
-
Expected processing times can vary based on the health plan’s guidelines.
-
Confirmation of receipt is typically provided by the health plan.
If a form is rejected, healthcare providers should know how to address common reasons for denial to facilitate resubmission effectively, particularly when dealing with the new york health plan form.
Ensuring Security and Compliance with the Prior Authorization Form
When handling sensitive patient information using the prior authorization form, securing this data is paramount. Healthcare providers must implement robust privacy and data protection measures to uphold HIPAA and GDPR compliance.
Utilizing platforms like pdfFiller can enhance security, thanks to features including 256-bit encryption and adherence to SOC 2 Type II standards, ensuring that patient data remains confidential.
Using pdfFiller to Complete Your Prior Authorization Pharmacy Benefit Request Form
pdfFiller simplifies the process of filling out and e-signing the prior authorization pharmacy benefit request form. Key features that enhance user experience include:
-
Document annotations and field validations to ensure all necessary information is provided.
-
PDF editing tools that allow for easy corrections and adjustments before submission.
Employing pdfFiller can provide a seamless and efficient experience for healthcare providers when navigating the details of the healthcare provider prescription form.
Real-Life Examples and Resources for the Prior Authorization Pharmacy Benefit Request Form
To facilitate understanding, healthcare providers may refer to examples of completed medication authorization forms that illustrate proper filling techniques. Additionally, various resources and guides related to the prior authorization process are available.
Testimonials and success stories from users of pdfFiller demonstrate how effective form completion can lead to successful authorization outcomes, showcasing the effectiveness of utilizing this technology.
How to fill out the NY Affinity Health Plan Prior Authorization
-
1.To access the Prior Authorization Pharmacy Benefit Request Form on pdfFiller, visit the pdfFiller website and use the search bar to find the form or navigate directly to the healthcare forms section.
-
2.Once you have located the form, click on it to open it in pdfFiller's editing interface. Familiarize yourself with the layout and the different fillable fields displayed on the form.
-
3.Before filling out the form, gather all necessary information including the patient's details, prescriber information, medication name, diagnosis codes, and any clinical justification documents like lab results.
-
4.Begin filling in the form by clicking on each fillable field. Enter the patient’s first name, last name, and date of birth accurately in the designated areas. Ensure all spelling is correct.
-
5.Continue by providing the prescriber’s details, including name, contact information, and required signature. Use the checkboxes for any applicable conditions or notes.
-
6.After completing all required fields, review the form carefully for any omitted information or errors. Ensure that all details align with the supporting documentation you have gathered.
-
7.Once finalized, save your changes in pdfFiller by clicking the ‘Save’ button or use the option to download the form as a PDF file to your device.
-
8.To submit the form, you can either upload it directly to the health plan's website or print it for mailing, depending on the submission guidelines.

Who is eligible to use the Prior Authorization Pharmacy Benefit Request Form?
The form is specifically for prescribers and healthcare providers in New York who need to request prior authorization for medication coverage from health plans.
Is there a deadline for submitting this form?
While specific deadlines vary by health plan, it is advisable to submit the Prior Authorization Pharmacy Benefit Request Form as soon as possible to ensure timely processing and medication access.
How should I submit the completed form?
You can submit the completed form through the health plan's online portal, by fax, or by mailing a printed copy. Check the specific submission guidelines provided by the health plan.
What supporting documents are required with this form?
Typically, supporting documents include clinical justification, such as lab results or medical records, that demonstrate the necessity of the medication requested in the form.
What common mistakes should I avoid when filling out this form?
Ensure all fields are filled out completely, double-check spelling for patient and prescriber information, and attach all necessary supporting documents to prevent delays.
How long does it take to process the Prior Authorization request?
Processing times can vary by health plan but usually take anywhere from a few days to a couple of weeks. It's essential to follow up with the health plan if you do not receive a response.
What if my request is denied?
If your prior authorization request is denied, the health plan will typically send a notification explaining the decision. You can appeal the denial with additional information or documentation showing the medical necessity.
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.