Last updated on Feb 20, 2026
Get the free reopened claims statement
Show details
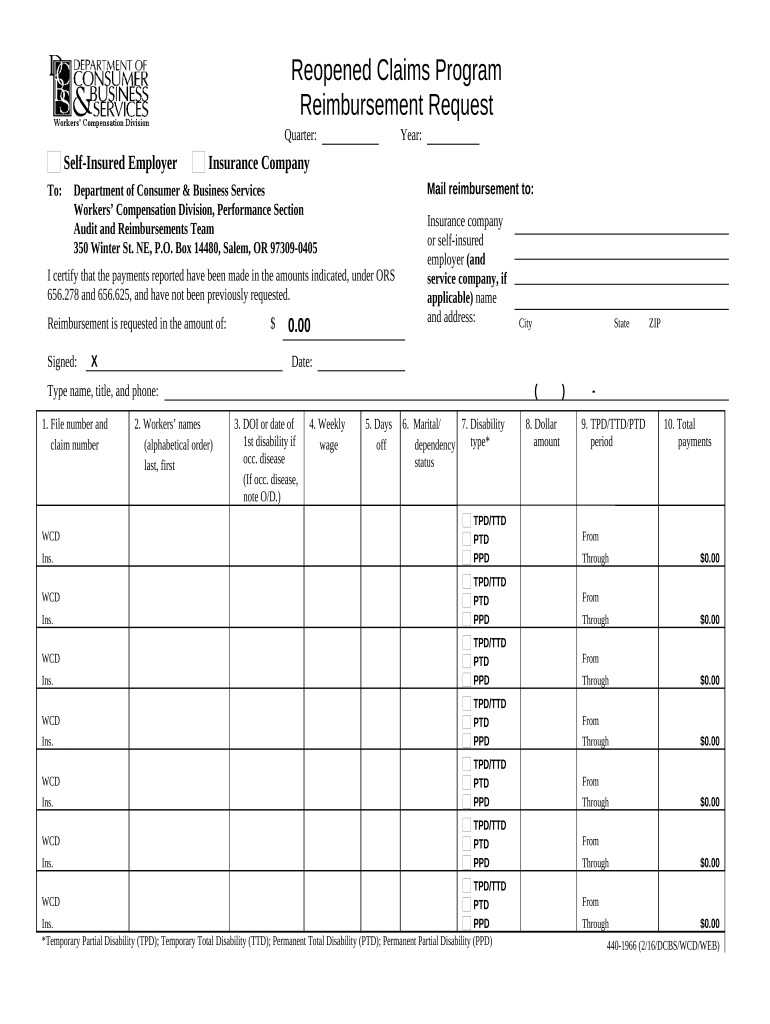
Reopened Claims Program Reimbursement Request Quarter Self-Insured Employer To Year Insurance Company Mail reimbursement to Department of Consumer Business Services Workers Compensation Division Performance Section Audit and Reimbursements Team 350 Winter St. NE P. O. Box 14480 Salem OR 97309-0405 I certify that the payments reported have been made in the amounts indicated under ORS 656. 278 and 656. 625 and have not been previously requested* Signed X or self-insured employer and service...company if applicable name and address WCD Ins* 2. Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D. 4. Weekly wage 5. Days off 6. Marital/ 7. Disability type dependency status 8. Dollar amount ZIP 9. TPD/TTD/PTD period TPD/TTD PTD PPD From Temporary Partial Disability TPD Temporary Total Disability TTD Permanent Total Disability PTD Permanent Partial Disability PPD State Date Type name title and phone 1. O. Box 14480 Salem OR 97309-0405 I...certify that the payments reported have been made in the amounts indicated under ORS 656. 278 and 656. 625 and have not been previously requested* Signed X or self-insured employer and service company if applicable name and address WCD Ins* 2. 278 and 656. 625 and have not been previously requested* Signed X or self-insured employer and service company if applicable name and address WCD Ins* 2. Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D....Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D. 4. Weekly wage 5. Days off 6. Marital/ 7. Disability type dependency status 8. Dollar amount ZIP 9. 4. Weekly wage 5. Days off 6. Marital/ 7. Disability type dependency status 8. Dollar amount ZIP 9. TPD/TTD/PTD period TPD/TTD PTD PPD From Temporary Partial Disability TPD Temporary Total Disability TTD Permanent Total Disability PTD Permanent Partial Disability PPD State Date Type name title...and phone 1. O. Box 14480 Salem OR 97309-0405 I certify that the payments reported have been made in the amounts indicated under ORS 656. 278 and 656. 625 and have not been previously requested* Signed X or self-insured employer and service company if applicable name and address WCD Ins* 2. Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D. 278 and 656. 625 and have not been previously requested* Signed X or self-insured employer and service...company if applicable name and address WCD Ins* 2. Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D. 4. Weekly wage 5. Days off 6. Marital/ 7. Disability type dependency status 8. Dollar amount ZIP 9. Workers names alphabetical order last first 3. DOI or date of 1st disability if occ* disease note O/D. 4. Weekly wage 5. Days off 6. Marital/ 7. Disability type dependency status 8. Dollar amount ZIP 9. TPD/TTD/PTD period TPD/TTD PTD PPD From...Temporary Partial Disability TPD Temporary Total Disability TTD Permanent Total Disability PTD Permanent Partial Disability PPD State Date Type name title and phone 1.
pdfFiller is not affiliated with any government organization
Fill out
Complete the form online in a simple drag-and-drop editor.
eSign
Add your legally binding signature or send the form for signing.
Share
Share the form via a link, letting anyone fill it out from any device.
Export
Download, print, email, or move the form to your cloud storage.
Why choose pdfFiller for your legal forms?
All-in-one solution
pdfFiller offers a PDF editor, eSignatures, file sharing, collaboration tools, and secure storage—all in one place.
Easy to use
pdfFiller is simple, cloud-based, has a mobile app, and requires no downloads or a steep learning curve.
Secure and compliant
With encryption, user authentication, and certifications like HIPAA, SOC 2 Type II, and PCI DSS, pdfFiller keeps sensitive legal forms secure.
What is reopened claims program reimbursement
The reopened claims program reimbursement is a financial process allowing recipients to receive payments for previously closed claims that have been adjusted or re-evaluated.
pdfFiller scores top ratings on review platforms
Easy to use, fast, organized
MAKE WORK MORE EASIER
easy to use
not interested in webinar
Very Easy to use.
it was good for what I needed
Who needs reopened claims statement template?
Explore how professionals across industries use pdfFiller.

Reopened claims statement template is needed by:
-
Insurance policyholders seeking reimbursement for adjusted claims.
-
Healthcare providers submitting claims for past services rendered.
-
Businesses needing reimbursement for previously denied claims.
Guide to reopened claims program reimbursement form on pdfFiller
TL;DR: How to fill out a reopened claims program reimbursement form
Completing a reopened claims program reimbursement form involves gathering necessary information about the claim, filling out each section accurately, and submitting the form in accordance with guidelines. Follow the step-by-step instructions provided in this guide to ensure a smooth filing process.
What is the reopened claims program?
The reopened claims program is designed to facilitate reimbursing employers for costs incurred due to previous workers' compensation claims that are reopened. Timeliness is crucial, as claims must be submitted promptly to comply with relevant regulations, including ORS 656.278 and 656.625, to avoid unnecessary complications.
-
Understand the conditions under which a claim can be reopened and the implications for employers involved.
-
Submit claims quickly to ensure you receive reimbursements without delays.
-
Familiarity with legal guidelines aids in proper claim handling, minimizing issues.
What information do you need for the reimbursement request?
Gathering accurate and complete information is critical for a successful reimbursement request. The reimbursement form requires details that represent the claim status and the employer's specifics.
-
Indicate when the claim is active or relevant for accurate record-keeping.
-
Insert accurate information about the self-insured employer responsible for the claim.
-
Provide correct mailing directions to ensure swift processing.
-
Ensure all necessary signatures and declarations are accurately filled in.
How do you fill out the reimbursement form step-by-step?
Filling out the reimbursement form is a straightforward process when you understand each section's requirements. The form consists of multiple sections that need careful attention.
-
Provide accurate personal details alongside the employer's information.
-
List all workers associated with the claim and their pertinent details.
-
Record the details surrounding the injury and corresponding weekly wage for verification.
-
Update claims with relevant numbers and payment details for processing.
What challenges may arise and how to overcome them?
Challenges can arise when information on the reimbursement form is missing or discrepancies are reported. Awareness of these potential pitfalls allows for better preparation.
-
Actively seek clarification from involved parties to fill in any gaps.
-
Establish a timeline for yourself to manage deadlines effectively.
-
Always double-check the form for completeness before submission.
What tools does pdfFiller offer for the reimbursement form?
pdfFiller provides a range of interactive tools that streamline the editing, signing, and management of the reimbursement form. These functionalities enhance collaboration and efficiency.
-
Utilize the intuitive interface to make edits and add signatures seamlessly.
-
Leverage cloud-based sharing features to work collaboratively on documents.
-
Access documents from anywhere, ensuring they are organized and retrievable.
What are the best practices for managing reopened claims?
Implementing best practices aids in effective management of reopened claims, ensuring that every step is documented and compliant with legal standards.
-
Develop a tracking system for monitoring the status of claims proactively.
-
Maintain meticulous records of all claims documentation for audits.
-
Ensure all procedures align with regulations to avoid legal contingencies.
How to fill out the reopened claims statement template
-
1.Log in to your pdfFiller account and navigate to the 'Forms' section.
-
2.Search for the 'Reopened Claims Program Reimbursement' form template.
-
3.Select the template and download it if necessary, or start filling it out online.
-
4.Begin with your personal information: fill in your name, address, and contact details at the top of the form.
-
5.Provide your claim number and date of the original claim in the designated fields.
-
6.Fill out the sections detailing the adjustments made to your claim, including the reasons for reopening the claim.
-
7.Attach any supporting documentation, such as explanation of benefits or adjustment letters, using the upload feature.
-
8.Review all entered information for accuracy before submission.
-
9.Submit the completed form electronically through pdfFiller, or print it to mail if required.
Related Forms







Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.