Last updated on Oct 18, 2014
Get the free Employee Medical Plan Enrollment Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
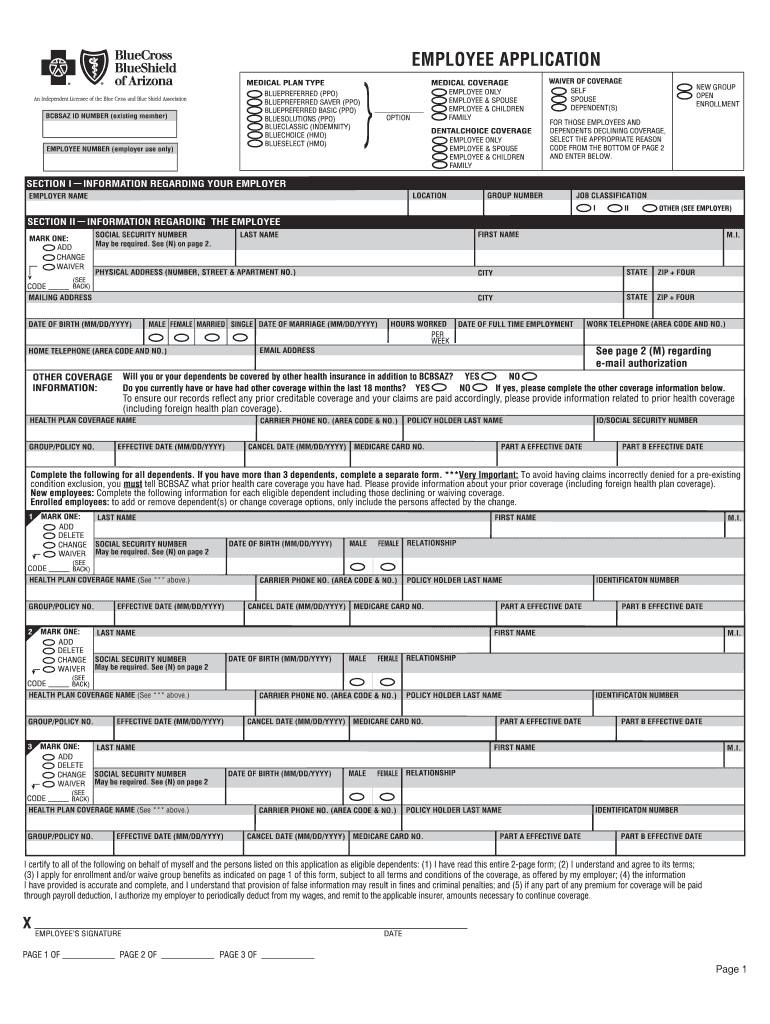
What is Medical Plan Form
The Employee Medical Plan Enrollment Form is a health insurance enrollment document used by employees to enroll in or waive health insurance coverage offered by their employer through Blue Cross Blue Shield of Arizona.
pdfFiller scores top ratings on review platforms
Who needs Medical Plan Form?
Explore how professionals across industries use pdfFiller.

Medical Plan Form is needed by:
-
Employees seeking health insurance coverage
-
Human Resources professionals managing employee benefits
-
Payroll departments handling health insurance enrollments
-
HR consultants advising on employee benefits programs
-
New hires needing to enroll in health plans
-
Employees wishing to waive health coverage
Comprehensive Guide to Medical Plan Form
Understanding the Employee Medical Plan Enrollment Form
The Employee Medical Plan Enrollment Form serves as a crucial document for employees wishing to enroll in or waive their health insurance coverage through their employer. This form is essential in facilitating the health insurance enrollment process, ensuring that employees can make informed decisions regarding their healthcare options. By properly completing the BCBSAZ health insurance form, employees streamline their enrollment or waiver process.
Purpose and Benefits of the Employee Medical Plan Enrollment Form
The primary purpose of the Employee Medical Plan Enrollment Form is to assist employees in navigating the health insurance enrollment or waiver process. Accurately filling out this form promotes timely processing of health insurance enrollments, which is vital for employees to secure their desired healthcare coverage. Using the Arizona employee benefits form correctly can lead to a smoother enrollment experience and help employees avoid potential delays.
Key Features of the Employee Medical Plan Enrollment Form
This form contains a variety of features designed to aid in the enrollment process. Key components include:
-
Multiple fillable fields for personal information and coverage selection.
-
Checkboxes for waiving coverage or selecting dependent enrollment options.
-
Certification requirements necessitating the employee's signature to affirm the accuracy of the provided information.
Understanding these features is vital for ensuring a complete and accurate submission.
Who Should Use the Employee Medical Plan Enrollment Form?
The target audience for the Employee Medical Plan Enrollment Form includes all employees in Arizona who aim to enroll in health insurance or waive their coverage. This form is also pertinent for those seeking to provide dependent coverage. It is crucial for employees to understand the options available and who needs to fill out the form to ensure comprehensive health coverage for themselves and their dependents.
How to Fill Out the Employee Medical Plan Enrollment Form Online
To complete the Employee Medical Plan Enrollment Form digitally, follow these steps:
-
Access the form using pdfFiller's online platform.
-
Gather necessary documents such as Personal Identification and existing health information.
-
Fill in the required fields, including personal information and coverage selections.
-
Review the information for accuracy before submission.
-
Submit the form electronically through the platform.
Having all relevant information ready beforehand will help streamline the process significantly.
Common Errors and How to Avoid Them When Completing the Form
Employees may frequently encounter errors when submitting the Employee Medical Plan Enrollment Form. Common mistakes include:
-
Leaving required fields blank.
-
Inaccurate personal information.
-
Failure to sign the certification section.
To ensure accuracy, refer to a checklist confirming that all sections are complete before submission. Avoiding these mistakes will lead to a smoother enrollment experience.
What Happens After You Submit the Employee Medical Plan Enrollment Form?
Once the Employee Medical Plan Enrollment Form is submitted, employees can expect the following:
-
Processing time, which may vary based on the employer's review timeline.
-
Receipt of confirmation acknowledging the form submission.
-
Ability to check the status of the submission through the employer's human resources department.
Understanding these steps can help manage expectations and ensure employees are informed about their enrollment status.
Security and Compliance Considerations for the Employee Medical Plan Enrollment Form
Handling sensitive information on the Employee Medical Plan Enrollment Form requires a focus on privacy and data protection. pdfFiller incorporates robust security features such as:
-
256-bit encryption to safeguard personal data.
-
Compliance with HIPAA and GDPR regulations.
-
Regular security audits to maintain data integrity.
By utilizing pdfFiller, users can ensure that their sensitive documents are protected throughout the enrollment process.
Utilizing pdfFiller for Your Employee Medical Plan Enrollment Form
Using pdfFiller offers several advantages when completing the Employee Medical Plan Enrollment Form. Key benefits include:
-
Easy editing and filling capabilities that simplify form completion.
-
eSigning options to ensure a quick submission process.
-
Cloud storage features for easy access to completed forms.
These features enhance the overall experience of filling out and submitting the form.
Your Next Steps to Complete the Employee Medical Plan Enrollment Form
Now is the perfect time to start filling out the Employee Medical Plan Enrollment Form using pdfFiller. The straightforward interface and available support make it easier to complete the form accurately and efficiently. Employees are encouraged to take advantage of this resource to secure their health coverage.
How to fill out the Medical Plan Form
-
1.Access the Employee Medical Plan Enrollment Form on pdfFiller by searching for the document title in the search bar after logging in.
-
2.Once the form is open, familiarize yourself with the sections. Locate fillable fields, checkboxes, and any instructional notes provided for guidance.
-
3.Gather necessary personal information, including your Social Security number, date of birth, and existing health insurance details, to complete the form accurately.
-
4.Begin filling out the form by entering your personal information in the designated fields. Take your time to ensure all entries are correct.
-
5.Select your desired health coverage options by checking the appropriate boxes. Be sure to review available plans provided by BCBSAZ.
-
6.If you have dependents, complete the section for dependent enrollment by adding their details as required. Ensure all information is accurate and up-to-date.
-
7.Review your entries thoroughly to confirm the accuracy of your information. Make use of the preview function in pdfFiller to check your responses.
-
8.Once satisfied, proceed to the signature field to certify the truthfulness of your information. Follow on-screen prompts to sign electronically.
-
9.Save your completed form regularly to avoid losing any changes. Use the 'Save' option in pdfFiller and consider downloading a copy for your records.
-
10.Finally, submit your form directly through pdfFiller if applicable, or download and send it to your HR department as instructed.

Who is eligible to use the Employee Medical Plan Enrollment Form?
The form is designed for all employees of organizations that offer health insurance coverage through Blue Cross Blue Shield of Arizona. Eligibility includes new hires and current employees wishing to enroll or waive insurance.
What is the deadline for submitting this enrollment form?
Deadlines for submission can vary by employer. It's recommended to submit the form as early as possible during the open enrollment period or immediately upon starting employment to ensure health coverage.
How can I submit the completed Employee Medical Plan Enrollment Form?
You can submit the completed form electronically through pdfFiller if your employer allows it, or by downloading it and emailing or handing it in to your HR department as per their submission guidelines.
What supporting documents are required with this form?
Typically, you will need to provide personal identification information, such as your Social Security number and any current health insurance details. Check with your HR department for any specific requirements.
What common mistakes should I avoid when completing the form?
Common mistakes include missing signatures, incorrect personal information, and failing to select the desired coverage options. Double-check all fields before submission to avoid delays.
How long does it take to process submitted enrollment forms?
Processing times can vary, but generally expect a response from your HR department within a few weeks. If there are any issues, they should notify you as soon as possible.
Can I make changes after submitting the form?
Changes may be possible, but they typically require re-submitting a corrected form. Be sure to check with your HR department for their specific policies regarding modifications to submitted enrollments.
Related Forms









If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.