Last updated on Oct 20, 2014

Get the free Patient Assistance Program Application
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Patient Assistance Form
The Patient Assistance Program Application is a healthcare form used by patients or their legal guardians to apply for financial assistance for prescription medications.
pdfFiller scores top ratings on review platforms
Who needs Patient Assistance Form?
Explore how professionals across industries use pdfFiller.

Patient Assistance Form is needed by:
-
Patients seeking financial aid for medications
-
Legal guardians completing applications for minors
-
Attending physicians certifying patient needs
-
Healthcare providers assisting patients with applications
-
Social workers supporting families in need
-
Pharmacists enrolling patients in assistance programs
Comprehensive Guide to Patient Assistance Form
Understanding the Patient Assistance Program Application
The Patient Assistance Program Application is a crucial form in healthcare, focusing on helping patients secure necessary medications they require. This application serves as a medication assistance form, facilitating financial aid to those in need. Through this program, eligible patients can obtain essential medications while alleviating financial stress.
Benefits of the Patient Assistance Program
Completing the Patient Assistance Program Application can lead to significant financial assistance for prescription medications. Patients who qualify benefit from reduced costs, allowing access to vital medications without the financial burden typically associated with them. This healthcare financial assistance form is specifically designed to support individuals facing economic hardships.
Eligibility Criteria for the Patient Assistance Program Application
Applicants must fulfill certain eligibility criteria that are critical for navigating the application process successfully. The basic requirements include patient demographics and income levels. To qualify, individuals must provide a patient income verification form detailing their financial circumstances, ensuring they meet the necessary criteria for assistance.
Key Features of the Patient Assistance Program Application
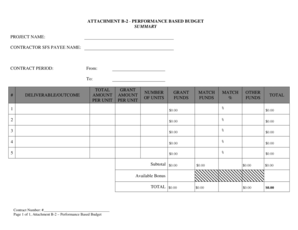
The Patient Assistance Program Application includes several important features essential for effective processing. Key aspects of this form involve required fields such as patient name, address, and contact information, and pertinent diagnostic information must be captured from the attending physician’s certification. Additionally, the prescription drug coverage form requires specific signatures to verify eligibility.
Who Needs to Complete the Patient Assistance Program Application?
Various stakeholders play a role in the application process, including patients, legal guardians, and attending physicians. Each party has specific responsibilities, and signatures from the patient or legal guardian, as well as the attending physician, are mandatory to validate the application. Understanding these roles ensures accuracy and compliance throughout the application process.
How to Fill Out the Patient Assistance Program Application Online (Step-by-Step)
-
Begin by accessing the application form on pdfFiller.
-
Fill in necessary personal details such as the patient's name and contact information.
-
Complete sections related to income and insurance details, including Medicare enrollment.
-
Attach required signatures from both the patient and the attending physician.
-
Review the completed form for accuracy before submission.
Submission Process for the Patient Assistance Program Application
Once the application is completed, submission to UCB, Inc. can be done through various delivery methods, including electronic submission via pdfFiller. It is important to be aware of potential fees and deadlines associated with the application process, as well as estimated processing times to ensure timely assistance.
What Happens After You Submit the Application?
After submission, applicants can track their application status through the provided channels by UCB. In the event of a rejection, understanding common rejection reasons can provide valuable insights for resubmission. Applicants should be prepared to follow through with the necessary steps to correct any issues and reapply for assistance.
Ensuring Security and Privacy with the Patient Assistance Program Application
pdfFiller prioritizes security during the document handling process, offering features such as 256-bit encryption and compliance with HIPAA and GDPR regulations. Protecting personal information is vital, and applicants must take care to safeguard sensitive data provided in the application to ensure their privacy is maintained throughout the process.
Get Started with pdfFiller for Your Patient Assistance Program Application Today
Leveraging pdfFiller’s capabilities allows users to fill out, edit, and eSign the Patient Assistance Program Application easily. With a user-friendly interface and robust security features, pdfFiller simplifies managing healthcare documents effectively, ensuring users can focus on receiving the help they need.
How to fill out the Patient Assistance Form
-
1.Access the Patient Assistance Program Application on pdfFiller. Simply visit the pdfFiller website and search for the form by its name.
-
2.Once you locate the form, click on it to open it in the pdfFiller editor. Familiarize yourself with the layout and sections of the form.
-
3.Before starting to fill out the form, gather all required information such as the patient's personal details, Medicare information, and household income.
-
4.Begin completing the form by entering the patient's first and last name, address, city, state, and zip code in the appropriate fields.
-
5.Proceed to fill in the contact number and birth date. Ensure the Social Security number and any identification numbers are accurate.
-
6.Include details about Medicare enrollment and the gross monthly household income of the applicant in their respective fields.
-
7.Utilize checkboxes where necessary, especially for certifying information related to the application.
-
8.Ensure the form is signed by both the patient or legal guardian and the attending physician. They will also need to provide diagnostic information.
-
9.After completing all fields, review the form for any errors or missing information, ensuring accuracy throughout.
-
10.Once thoroughly reviewed, save your progress. You can choose to download a copy for your records or submit it directly through pdfFiller.
-
11.Finalize by following the prompts for submission, which may include mailing the completed form to UCB, Inc. for review.

Who is eligible to apply using this form?
Patients requiring financial assistance for prescription medications or their legal guardians can use this form. Eligibility extends to those with limited income or without full prescription drug coverage.
What documents do I need to provide with the application?
Applicants typically need to provide proof of income, Medicare enrollment details, and any relevant identification numbers. Ensure all required fields are completed on the form for efficient processing.
How do I submit the completed application?
After filling out the application, you can submit it by mailing the printed copy to UCB, Inc. Follow any specific submission instructions provided at the end of the form.
How long will it take to process my application?
Processing times can vary. It's recommended to allow several weeks for the review process. For specific timelines, contact UCB, Inc. directly.
Can I fill out this form electronically?
Yes, the form can be completed electronically using pdfFiller, which allows users to fill, save, and submit online, streamlining the application process.
What common mistakes should I avoid when filling out this form?
Common errors include missing signatures, incorrect personal information, and not providing required supporting documents. Double-check all entries to ensure accuracy.
Are there any fees associated with applying for assistance?
Submitting the Patient Assistance Program Application should not incur fees. However, verify with UCB, Inc. if there are any associated charges for the services being requested.
Related Forms






If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.