Last updated on Apr 10, 2026
FL form Orthopaedic Institute Authorization to Disclose free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is FL form Orthopaedic Institute Authorization to Disclose
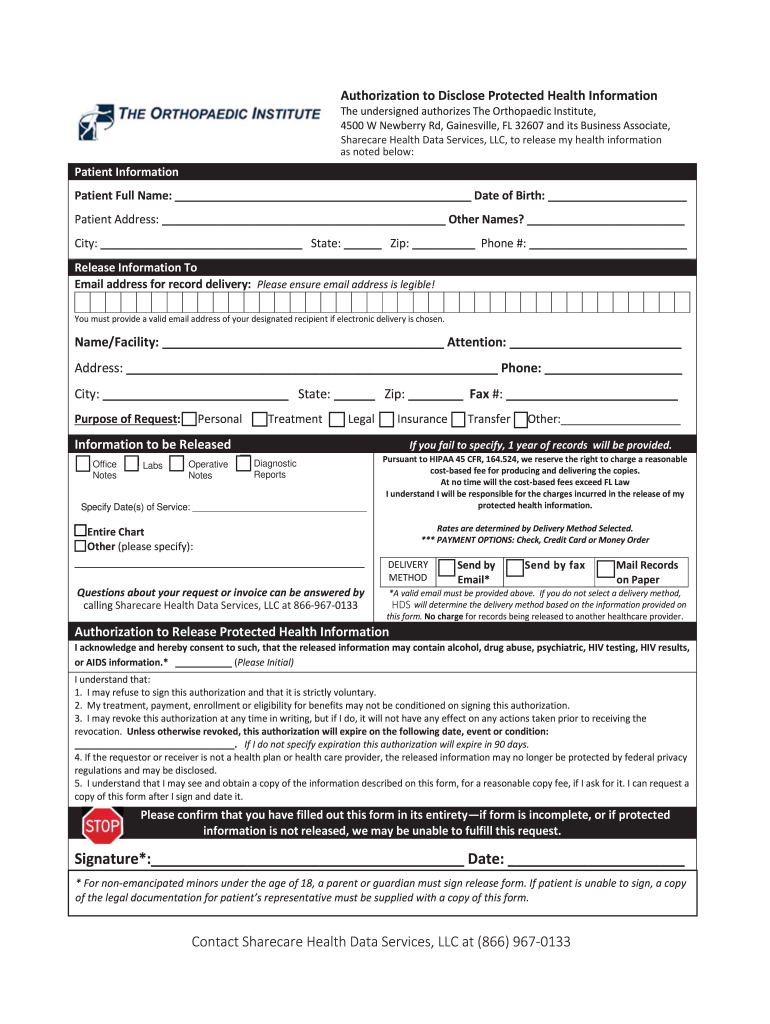
The Authorization to Disclose Protected Health Information is a legal document used by patients to grant permission for the release of their protected health information to designated recipients.
pdfFiller scores top ratings on review platforms
Who needs FL form Orthopaedic Institute Authorization to Disclose?
Explore how professionals across industries use pdfFiller.

FL form Orthopaedic Institute Authorization to Disclose is needed by:
-
Patients seeking to share their health information.
-
Parents or guardians needing access to a minor's medical records.
-
Healthcare providers requiring authorization to disclose patient data.
-
Insurance companies needing patient information for claims processing.
-
Lawyers or legal representatives managing health-related cases.
Comprehensive Guide to FL form Orthopaedic Institute Authorization to Disclose
What is the Authorization to Disclose Protected Health Information?
The Authorization to Disclose Protected Health Information is a crucial document that enables patients and their guardians to permit the release of sensitive health information. This form serves to ensure compliance with the Health Insurance Portability and Accountability Act (HIPAA), which regulates the sharing of protected health information among healthcare entities. Typically, this authorization form is utilized by patients, parents, and guardians seeking to manage their medical records and personal health data.
Purpose and Benefits of the Authorization to Disclose Protected Health Information
This form empowers patients and their guardians by providing a clear mechanism for controlling the dissemination of their health information. One of the primary benefits of using the authorization form is the assurance of confidentiality and adherence to HIPAA regulations. Additionally, there are specific scenarios in which the form is essential, such as when transferring medical records between healthcare providers or sharing information with specialists.
Key Features of the Authorization to Disclose Protected Health Information
The structure of the Authorization to Disclose Protected Health Information is designed to be user-friendly and comprehensive. Key features include:
-
Fillable fields for essential patient details such as Full Name and Date of Birth.
-
Checkbox options to select desired delivery methods and specific purposes for the release.
-
Security measures implemented to comply with HIPAA, ensuring that the information shared remains confidential.
Who Needs the Authorization to Disclose Protected Health Information?
This form can be requested by patients or their guardians. It is crucial for individuals who wish to grant access to their health information to various healthcare professionals, such as doctors, insurers, and hospitals. For example, when a patient transitions to a new healthcare provider or seeks specialized treatment, they must authorize the release of their medical records to facilitate continuity of care.
How to Fill Out the Authorization to Disclose Protected Health Information Online (Step-by-Step)
Filling out the authorization form online is a straightforward process. Here are the steps to complete the form:
-
Access the authorization form through a secure platform.
-
Enter the Patient Full Name, Date of Birth, and other required fields.
-
Select the delivery methods and purposes of the request using the checkboxes provided.
-
Review all entered information for accuracy before submission.
-
Submit the completed form via the chosen delivery method.
Common errors to avoid include missing required fields or providing incorrect personal information.
Submission Methods and Delivery Options for the Authorization to Disclose Protected Health Information
Once the authorization form is completed, there are several submission methods available:
-
Online submission through a secure portal.
-
Mailing a printed copy to the designated recipient.
-
Delivering the form in person to the healthcare provider’s office.
Choosing the right delivery method depends on the urgency of the request and personal preference. Additionally, users should consider options for tracking their submission to confirm receipt.
Security and Compliance Considerations for the Authorization to Disclose Protected Health Information
Data security is paramount when dealing with health information. pdfFiller implements advanced security measures, including 256-bit encryption and adherence to HIPAA regulations, assuring users that their sensitive information is adequately protected. Safeguarding personal health information should always be a priority, and pdfFiller demonstrates a continuous commitment to data protection.
What Happens After You Submit the Authorization to Disclose Protected Health Information?
After submitting the authorization form, users can expect a defined process. Typically, the timeframe for processing requests varies, but healthcare providers aim to respond promptly. Follow-up actions may include receiving confirmation of receipt or further instructions from the healthcare provider. Users can also check the status of their submitted authorization for peace of mind.
How to Download and Save the Authorization to Disclose Protected Health Information PDF
Once the form has been filled out, downloading and saving the completed authorization is simple. Follow these steps:
-
Locate the download option on the pdfFiller platform.
-
Save the document in a secure digital format.
-
Ensure that a copy is stored in a safe place for personal records.
Maintaining a saved copy of the authorization is essential for future reference and personal management of health information.
Empowering Your Healthcare Journey with pdfFiller
pdfFiller provides an efficient, user-friendly platform for filling out forms like the Authorization to Disclose Protected Health Information. With advanced features for editing and securely managing documents, users can take control of their healthcare records. Start using pdfFiller today to streamline your health information management.
How to fill out the FL form Orthopaedic Institute Authorization to Disclose
-
1.To access the Authorization to Disclose Protected Health Information form, visit pdfFiller and search for the form by its official name.
-
2.Once you find the form, click to open it in the pdfFiller editor. Here, you will be able to navigate through the fillable fields.
-
3.Before starting, gather necessary information such as the patient's full name, date of birth, address, and the names of recipients for the health information.
-
4.Begin completing the form by filling in the patient's details in the designated fields. Ensure all entries are accurate to avoid delays.
-
5.Use the checkboxes to select the desired delivery methods and the purpose of the request according to your needs.
-
6.Once all fields are completed, take a moment to review the form for any errors or missing information. This step is crucial to ensure smooth processing.
-
7.Finalize the form by providing your signature in the appropriate field, indicating your consent for the information disclosure.
-
8.After finalizing, save your progress on pdfFiller. You can download the form to your device or submit it directly through the platform.

Who is eligible to use this form?
Patients, parents, or guardians can use the Authorization to Disclose Protected Health Information form. It is designed for anyone needing to authorize the release of protected health information.
Are there any deadlines for submitting this form?
Timeliness can vary based on the request and recipient. It is best to submit the form as soon as possible to avoid delays in accessing your health information.
How should I submit the completed form?
You can submit the completed Authorization to Disclose Protected Health Information form by downloading it and sending it directly to the specified recipients or uploading it through the relevant platform.
What supporting documents do I need?
Typically, you may need to provide identification or proof of guardianship along with the completed form to verify your identity and authority.
What are common mistakes to avoid when filling out this form?
Common mistakes include omitting critical information such as the patient's details or failing to sign the form. Double-check all fields to avoid processing delays.
How long does it take to process this authorization?
Processing times can vary based on the recipient's response time. It's advisable to follow up if you haven't received confirmation within a reasonable period after submission.
Can I revoke my authorization after it's submitted?
Yes, you have the right to revoke your authorization at any time. You may need to submit a revocation form to the same entities you initially authorized.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.