Last updated on Mar 29, 2026
Medical Bill Receipt free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
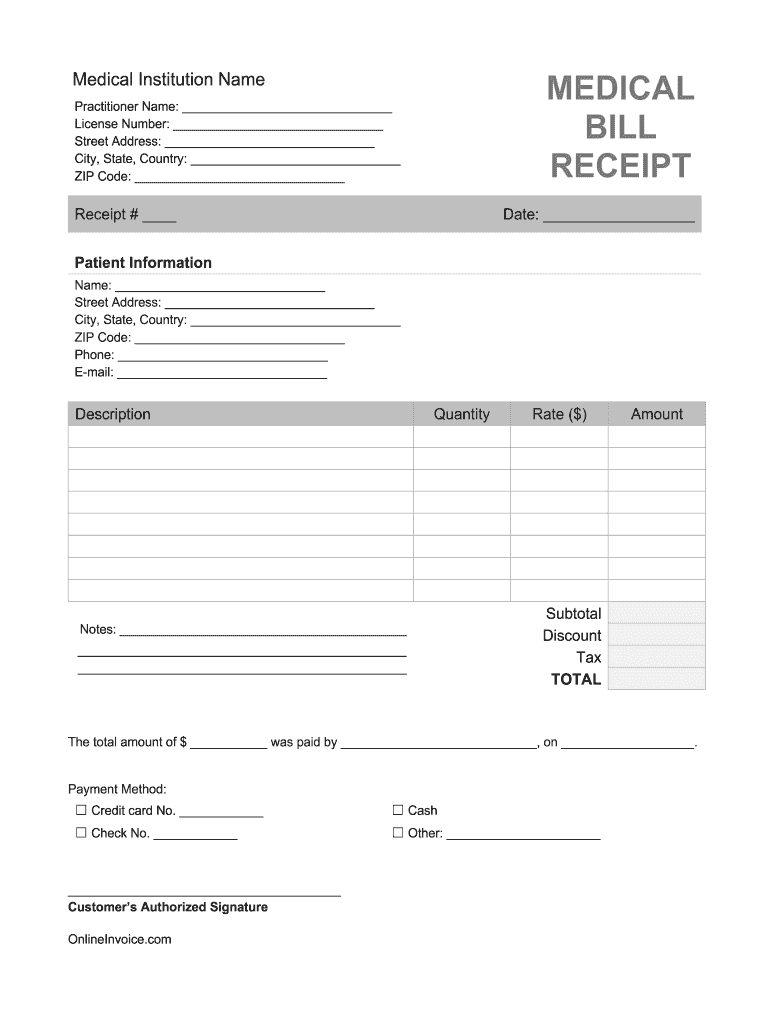
What is Medical Bill Receipt
The Medical Billing Receipt Template is a document used by healthcare practitioners to record payments received from patients, facilitating accurate financial documentation.
pdfFiller scores top ratings on review platforms
I looked on line a long time to find a program where I can enter info for W2c, etc. & this is a great program. It offers many different areas, choices to work with.
I love this program. It is user friendly and produces a quality document.
Who needs Medical Bill Receipt?
Explore how professionals across industries use pdfFiller.

Medical Bill Receipt is needed by:
-
Healthcare practitioners managing patient billing
-
Medical offices requiring payment documentation
-
Patients needing proof of payment for services
-
Insurance companies verifying medical charges
-
Accountants handling healthcare billing records
Comprehensive Guide to Medical Bill Receipt
What is the Medical Billing Receipt Template?
The Medical Billing Receipt Template is a vital document used in healthcare practices to accurately record payments received from patients. This template includes essential components such as practitioner and patient information, ensuring that all relevant details are documented for financial tracking purposes. Each element within the template plays a crucial role in maintaining clear records of financial transactions.
Purpose and Benefits of the Medical Billing Receipt Template
Accurate documentation of patient payments is essential for maintaining financial records in healthcare settings. By utilizing a medical billing receipt template, healthcare practitioners benefit from enhanced efficiency and professionalism in their billing processes. This form serves as an official record for patients, ensuring transparency and fostering trust.
Key Features of the Medical Billing Receipt Template
The template is designed with various features that facilitate easy use. Key elements include:
-
Fillable fields allowing for clear input of patient and practitioner details
-
Checkboxes to indicate services rendered or items charged
-
An authorization signature line for validation
-
A detailed breakdown of charges and payment information
Who Needs the Medical Billing Receipt Template?
This template is essential for a range of healthcare providers including doctors, clinics, and hospitals. It helps streamline the billing process by providing a structured format for billing patients and coordinating with insurance companies. By utilizing this template, practitioners can ensure compliance and accuracy in their financial interactions.
How to Fill Out the Medical Billing Receipt Template Online (Step-by-Step)
To complete the medical billing receipt template online using pdfFiller, follow these steps:
-
Open the medical billing receipt template in pdfFiller.
-
Fill in the required fields, including practitioner and patient information.
-
Check the applicable boxes for services provided.
-
Review the breakdown of charges carefully.
-
Sign the document using the digital signature feature.
-
Save the completed form for future reference.
Common Errors and How to Avoid Them
When filling out the medical billing receipt template, common errors include incorrect patient details and missing signatures. To avoid these mistakes, consider the following tips:
-
Double-check all entered information for accuracy.
-
Ensure that all required fields are filled out completely.
-
Review the template before submission to catch any overlooked details.
How to Sign the Medical Billing Receipt Template
Signing the medical billing receipt template can be done using either a digital signature or a wet signature, depending on your preference and requirements. With pdfFiller, users can benefit from enhanced security features that ensure the integrity of signed documents, making the signing process both efficient and secure.
How to Download and Save the Medical Billing Receipt Template PDF
Once you have filled out the medical billing receipt template, it is important to save it properly. To do this:
-
Select the "Download" option in pdfFiller after completing the form.
-
Choose the desired file format for saving.
-
Store the document in an organized manner for easy access in the future.
Submission Methods for the Medical Billing Receipt Template
Upon completing the medical billing receipt template, it can be submitted through various methods. Options include sending directly to patients or submitting to insurance companies. Be aware of any potential fees or processing times associated with these submissions to ensure timely payments.
Utilizing pdfFiller for Your Medical Billing Receipt Template Needs
PdfFiller offers a range of features tailored to support users in creating and managing their medical billing receipts. With robust security and compliance measures in place for handling sensitive documents, pdfFiller ensures that your data is protected while you create professional billing receipts.
How to fill out the Medical Bill Receipt
-
1.To begin, access pdfFiller and locate the Medical Billing Receipt Template by using the search bar.
-
2.Once found, click on the template to open it in the pdfFiller editor, where you will see the fillable fields clearly outlined.
-
3.Before you start filling out the form, gather all necessary information such as practitioner name, patient details, and payment amounts to ensure accuracy.
-
4.Navigate through the form by clicking on each fillable field. You can type directly into these areas, allowing for easy data entry.
-
5.Fill in the 'Practitioner Name' at the designated field using the text input feature provided by pdfFiller.
-
6.Next, input the 'Patient Information' including the patient's name, address, and contact details in the appropriate fields.
-
7.Detail the breakdown of charges by filling in the itemized list of services provided and their corresponding costs.
-
8.After you enter the payment details, including the payment method and amount received, review all entered information for completeness.
-
9.Utilize the signature feature to add the required signature in the designated line labeled 'Customer’s Authorized Signature'.
-
10.Once all fields are filled and verified for accuracy, finalize your document using the review tool available in pdfFiller.
-
11.After reviewing, click on the save option to store your document securely on pdfFiller.
-
12.You can download the completed form to your device or share it directly through email or submission options provided by pdfFiller.

Who can use the Medical Billing Receipt Template?
The Medical Billing Receipt Template can be used by healthcare practitioners, medical office staff, and patients needing proof of payment. It's essential for any entity involved in managing or verifying healthcare payments.
Are there any deadlines associated with using this form?
While there are no specific deadlines for filling out the Medical Billing Receipt Template itself, it's crucial to provide receipts promptly to ensure timely insurance claims and patient records.
What methods are available for submitting this form?
This form can be submitted through various methods, including direct email, print, or online submission, depending on your specific practices and regulations. Ensure to check with your office protocols.
What information is required to complete the form?
To complete the Medical Billing Receipt Template, you will need the practitioner's name, patient information, a breakdown of services provided, payment details, and an authorized signature.
What are some common mistakes to avoid while filling out this form?
Common mistakes include entering incorrect amounts, omitting patient information, or failing to obtain an authorized signature. Always double-check for accuracy.
How quickly can I expect processing after submitting this form?
Processing times can vary based on the healthcare provider’s practices. Typically, expect confirmations and record updates within a few business days after submission.
Do I need to notarize this receipt?
No, notarization is not required for the Medical Billing Receipt Template. However, obtaining a signature from the patient is necessary for authorization.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.